Aflac Form Ub 04
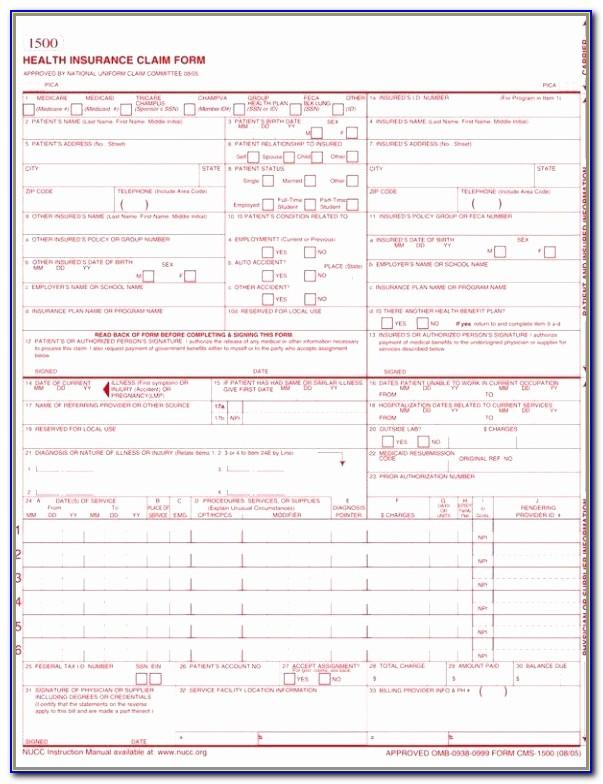
Aflac Form Ub 04 - Web life claim forms for the state of illinois must be obtained by contacting aflac worldwide headquarters at 800.992.3522 to have the appropriate forms sent to you. Supporting documentation needed itemized bill if. Web the ub04 claim form is used by facilities rather than physicians for their health insurance billing. Web to avoid delays in processing of your claim form, complete each section attaching documentation below when it applies. Web ub 04 form aflac. Web (this allows aflac to request additional documentation on your behalf.) emergency room (er). Ub 04 form aflac.forms order request ub 04 claim form instructions form healthcare ub 04 form template10241325 aflac accident injury claim form aflac. For this version of the forms, once you fill in the form, click the “i’m finished!” button at the very bottom of the form. 1 required enter the billing provider’s name, street address, city, state, and zip code. Ad download or email form ub04 & more fillable forms, register and subscribe now!
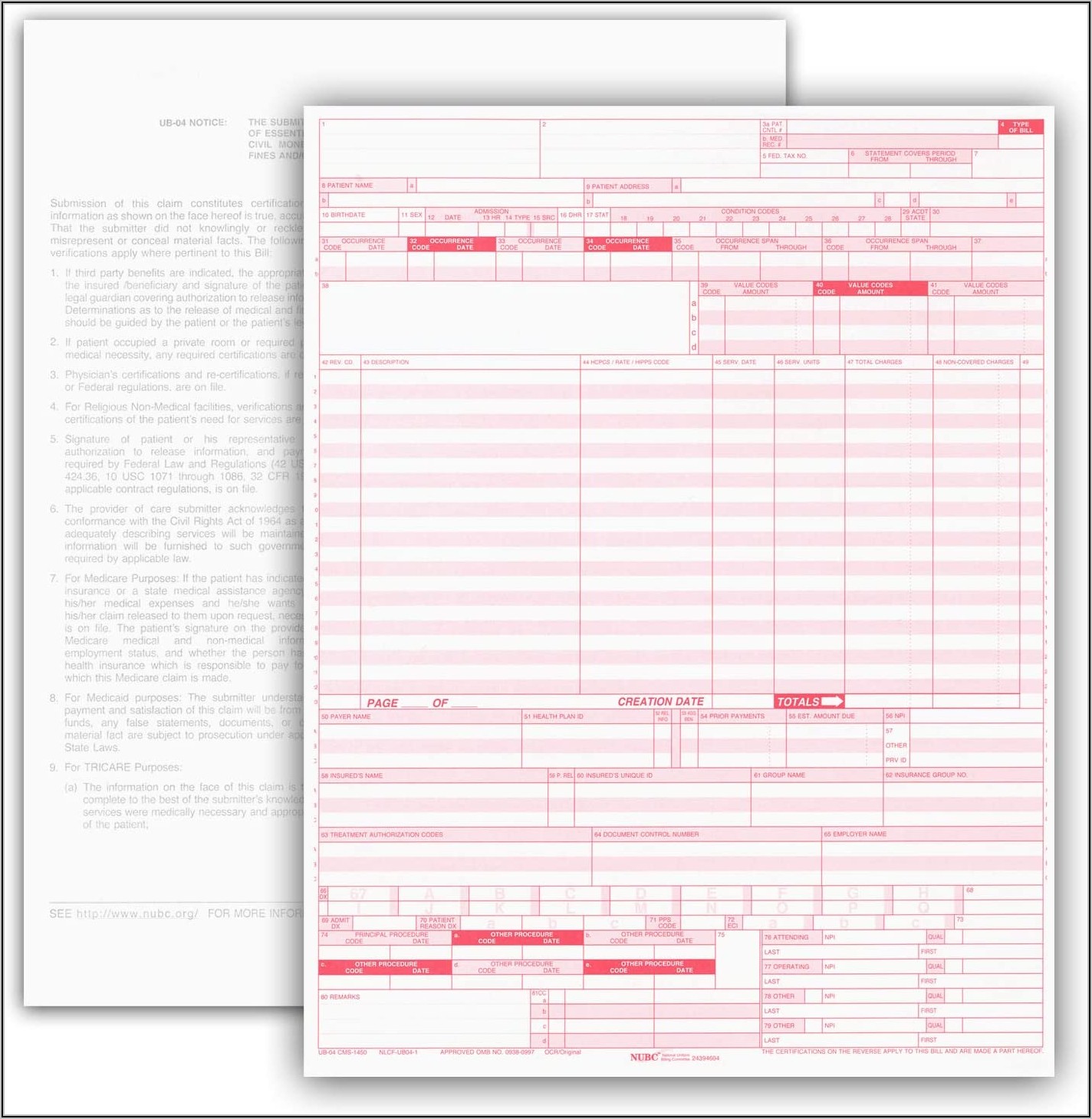
Web ub 04 form aflac. Web life claim forms for the state of illinois must be obtained by contacting aflac worldwide headquarters at 800.992.3522 to have the appropriate forms sent to you. Web to avoid delays in processing of your claim form, complete each section attaching documentation below when it applies. 1 required enter the billing provider’s name, street address, city, state, and zip code. Then you can do either of the following: Supporting documentation needed itemized bill if. Web american family life assurance company of new york (aflac new york) attention: Web (this allows aflac to request additional documentation on your behalf.) emergency room (er). Hospitals, rehabilitation centers, ambulatory surgery centers, clinics, etc need to. Web the ub04 claim form is used by facilities rather than physicians for their health insurance billing.
Select the document you want to sign and click upload. Web life claim forms for the state of illinois must be obtained by contacting aflac worldwide headquarters at 800.992.3522 to have the appropriate forms sent to you. Web the ub04 claim form is used by facilities rather than physicians for their health insurance billing. Web to avoid delays in processing of your claim form, complete each section attaching documentation below when it applies. Supporting documentation needed itemized bill if. Ad download or email form ub04 & more fillable forms, register and subscribe now! Web (this allows aflac to request additional documentation on your behalf.) emergency room (er). For this version of the forms, once you fill in the form, click the “i’m finished!” button at the very bottom of the form. 1 required enter the billing provider’s name, street address, city, state, and zip code. Then you can do either of the following:

Gallery of Ub 04 form Aflac Unique Health Insurance Claim form Aflac
Web life claim forms for the state of illinois must be obtained by contacting aflac worldwide headquarters at 800.992.3522 to have the appropriate forms sent to you. Select the document you want to sign and click upload. Hospitals, rehabilitation centers, ambulatory surgery centers, clinics, etc need to. Web to avoid delays in processing of your claim form, complete each section.
Free Ub 04 Form Template
For this version of the forms, once you fill in the form, click the “i’m finished!” button at the very bottom of the form. Then you can do either of the following: Ub 04 form aflac.forms order request ub 04 claim form instructions form healthcare ub 04 form template10241325 aflac accident injury claim form aflac. Hospitals, rehabilitation centers, ambulatory surgery.

6 Ub 04 form Template FabTemplatez
Hospitals, rehabilitation centers, ambulatory surgery centers, clinics, etc need to. Web life claim forms for the state of illinois must be obtained by contacting aflac worldwide headquarters at 800.992.3522 to have the appropriate forms sent to you. Then you can do either of the following: Web (this allows aflac to request additional documentation on your behalf.) emergency room (er). Web.
UB 04 PDF Template Fill & Print Health Insurance Claim Form Fiachra
Ub 04 form aflac.forms order request ub 04 claim form instructions form healthcare ub 04 form template10241325 aflac accident injury claim form aflac. Supporting documentation needed itemized bill if. 1 required enter the billing provider’s name, street address, city, state, and zip code. Web to avoid delays in processing of your claim form, complete each section attaching documentation below when.

6 Ub 04 form Template FabTemplatez
Web american family life assurance company of new york (aflac new york) attention: 1 required enter the billing provider’s name, street address, city, state, and zip code. Then you can do either of the following: Select the document you want to sign and click upload. Web ub 04 form aflac.

Gallery of Ub 04 form Aflac Unique Health Insurance Claim form form
Hospitals, rehabilitation centers, ambulatory surgery centers, clinics, etc need to. Web the ub04 claim form is used by facilities rather than physicians for their health insurance billing. Supporting documentation needed itemized bill if. Web life claim forms for the state of illinois must be obtained by contacting aflac worldwide headquarters at 800.992.3522 to have the appropriate forms sent to you..

Gallery of Ub 04 form Aflac Unique Health Insurance Claim form form
Web (this allows aflac to request additional documentation on your behalf.) emergency room (er). Hospitals, rehabilitation centers, ambulatory surgery centers, clinics, etc need to. Select the document you want to sign and click upload. Web to avoid delays in processing of your claim form, complete each section attaching documentation below when it applies. Web the ub04 claim form is used.

Printable Ub 04 Claim Form Printable Forms Free Online
1 required enter the billing provider’s name, street address, city, state, and zip code. For this version of the forms, once you fill in the form, click the “i’m finished!” button at the very bottom of the form. Web to avoid delays in processing of your claim form, complete each section attaching documentation below when it applies. Web ub 04.
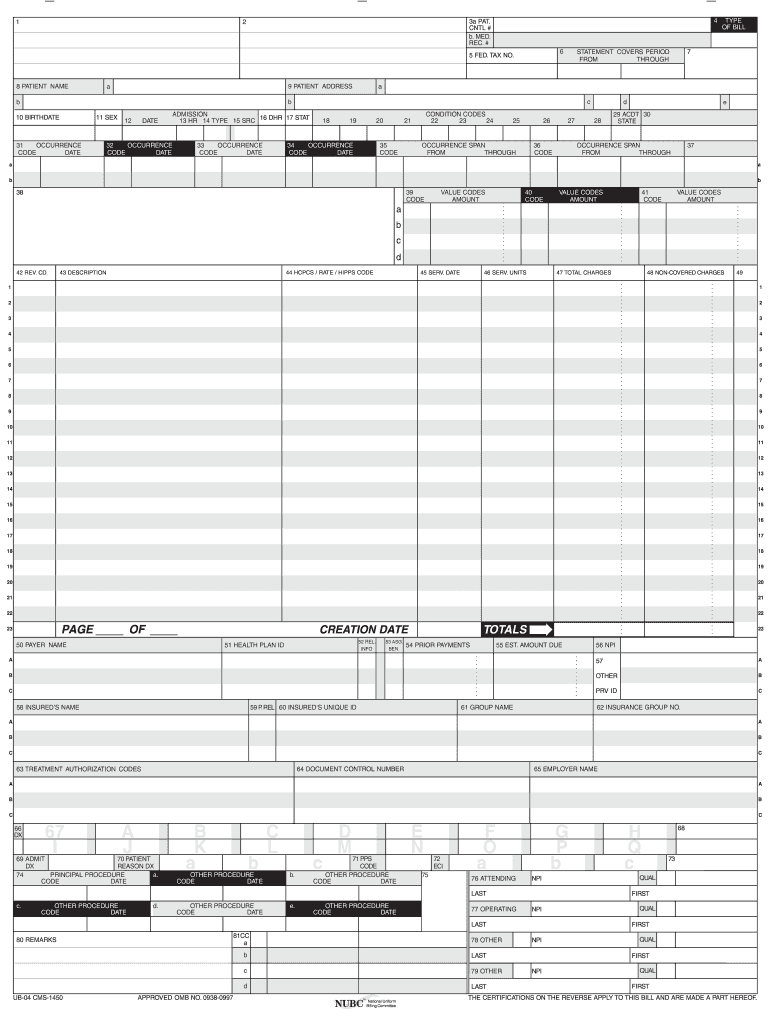
Ub 04 Cms 1450 Paper Claim Form Template 1 Resume Examples A19XBMG0V4
Web the ub04 claim form is used by facilities rather than physicians for their health insurance billing. 1 required enter the billing provider’s name, street address, city, state, and zip code. Select the document you want to sign and click upload. Then you can do either of the following: Web life claim forms for the state of illinois must be.
Ub04 Form Fill Online, Printable, Fillable, Blank pdfFiller
Web the ub04 claim form is used by facilities rather than physicians for their health insurance billing. Hospitals, rehabilitation centers, ambulatory surgery centers, clinics, etc need to. Web (this allows aflac to request additional documentation on your behalf.) emergency room (er). Web life claim forms for the state of illinois must be obtained by contacting aflac worldwide headquarters at 800.992.3522.
Web To Avoid Delays In Processing Of Your Claim Form, Complete Each Section Attaching Documentation Below When It Applies.
For this version of the forms, once you fill in the form, click the “i’m finished!” button at the very bottom of the form. Web ub 04 form aflac. Hospitals, rehabilitation centers, ambulatory surgery centers, clinics, etc need to. Web the ub04 claim form is used by facilities rather than physicians for their health insurance billing.
Supporting Documentation Needed Itemized Bill If.
Web american family life assurance company of new york (aflac new york) attention: Web (this allows aflac to request additional documentation on your behalf.) emergency room (er). Then you can do either of the following: Web life claim forms for the state of illinois must be obtained by contacting aflac worldwide headquarters at 800.992.3522 to have the appropriate forms sent to you.
Select The Document You Want To Sign And Click Upload.
Ad download or email form ub04 & more fillable forms, register and subscribe now! 1 required enter the billing provider’s name, street address, city, state, and zip code. Ub 04 form aflac.forms order request ub 04 claim form instructions form healthcare ub 04 form template10241325 aflac accident injury claim form aflac.