Ambetter Provider Appeal Form
Ambetter Provider Appeal Form - All fields are required information. Claim reconsideration claim appeal authorization appeal provider name. Web appeal by phone, fax, or in person. Reference materials 2023 provider & billing manual (pdf) 2022 provider & billing. Web to ensure that ambetter member's rights are protected, all ambetter members are entitled to a complaint/grievance and appeals process. Web appeal you file an appeal in response to a denial received from ambetter from health net. An appeal is the mechanism which allows providers the right to appeal actions of ambetter such. Web provider request for reconsideration and claim dispute form use this form as part of the ambetter from sunshine health request for reconsideration and. This could be a denial of coverage for requested medical care or for a claim you filed for. Use your zip code to find your personal plan.
See coverage in your area; Claim reconsideration claim appeal authorization appeal provider name. You must file an appeal within 180 days of the date on the denial letter. Web provider reconsideration and appeal request form use this form to request one of the following: Web outpatient prior authorization fax form (pdf) outpatient treatment request form (pdf) provider fax back form (pdf) applied behavioral analysis authorization form (pdf). Use your zip code to find your personal plan. The claim dispute must be submitted within. Web appeal you file an appeal in response to a denial received from ambetter from health net. Claim complaints must follow the dispute process and then the complaint process below. Web all ambetter from arizona complete health members are entitled to a complaint/grievance and appeals process if a member is displeased with any aspect of services rendered.
Web use this form as part of the ambetter from superior healthplanrequest for reconsideration and claim dispute process. The requesting physician must complete an authorization request using one of the following methods: Web all ambetter from arizona complete health members are entitled to a complaint/grievance and appeals process if a member is displeased with any aspect of services rendered. Claim reconsideration claim appeal authorization appeal provider name. Web to ensure that ambetter member's rights are protected, all ambetter members are entitled to a complaint/grievance and appeals process. The completed form can be returned by mail or fax. Web outpatient prior authorization fax form (pdf) outpatient treatment request form (pdf) provider fax back form (pdf) applied behavioral analysis authorization form (pdf). Web appeal you file an appeal in response to a denial received from ambetter from health net. Disputes of denials for code editing policy. Web use this form as part of the ambetter from coordinated care claim dispute/appeal process to dispute the decision made during the request for reconsideration process.
Texas Bcbs Provider Appeal Fill Out and Sign Printable PDF Template
The requesting physician must complete an authorization request using one of the following methods: Web to ensure that ambetter member's rights are protected, all ambetter members are entitled to a complaint/grievance and appeals process. Web appeal by phone, fax, or in person. Web provider request for reconsideration and claim dispute form use this form as part of the ambetter from.
Wellcare Appeal Form Fill Online, Printable, Fillable, Blank pdfFiller
The procedures for filing a. The requesting physician must complete an authorization request using one of the following methods: Web all ambetter from arizona complete health members are entitled to a complaint/grievance and appeals process if a member is displeased with any aspect of services rendered. Web as an ambetter network provider, you can rely on the services and support.
Form 2349 Download Fillable PDF or Fill Online Second Level Appeal of
Claim reconsideration claim appeal authorization appeal provider name. Claim complaints must follow the dispute process and then the complaint process below. Web use this form as part of the ambetter from coordinated care claim dispute/appeal process to dispute the decision made during the request for reconsideration process. Web ambetter provider reconsiderations, disputes and complaints (cc.um.05.01) to see if the case.
Buckeye Waiver Fill Out and Sign Printable PDF Template signNow
Web use this form as part of the ambetter from coordinated care claim dispute/appeal process to dispute the decision made during the request for reconsideration process. The requesting physician must complete an authorization request using one of the following methods: Web outpatient prior authorization fax form (pdf) outpatient treatment request form (pdf) provider fax back form (pdf) applied behavioral analysis.
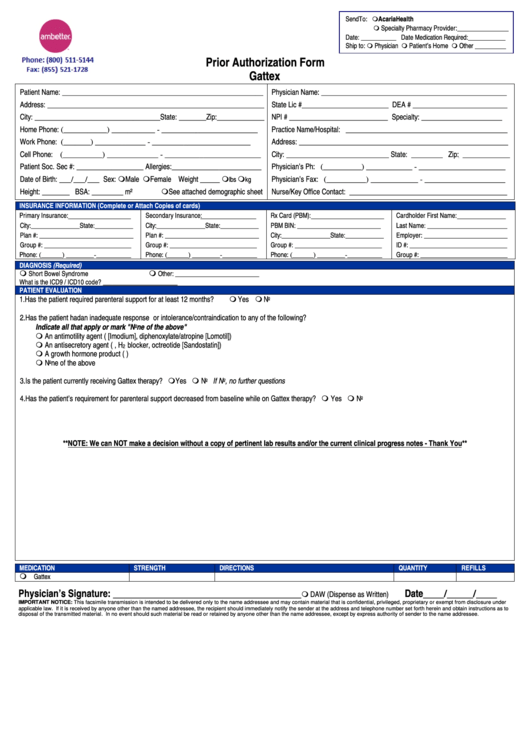
Ambetter Prior Authorization Form Gattex printable pdf download
Log in to the nch provider web portal at. The completed form can be returned by mail or fax. Web use this form as part of the ambetter from superior healthplanrequest for reconsideration and claim dispute process. Claim complaints must follow the dispute process and then the complaint process below. Reference materials 2023 provider & billing manual (pdf) 2022 provider.

Free Arkansas Medicaid Prior (Rx) Authorization Form PDF eForms
Web appeal by phone, fax, or in person. Reference materials 2023 provider & billing manual (pdf) 2022 provider & billing. Web use this form as part of the ambetter from superior healthplanrequest for reconsideration and claim dispute process. This could be a denial of coverage for requested medical care or for a claim you filed for. Claim reconsideration claim appeal.

Envolve Vision Newsletter Volume 6 Issue 3 National English
Disputes of denials for code editing policy. Use your zip code to find your personal plan. Web to ensure that ambetter member's rights are protected, all ambetter members are entitled to a complaint/grievance and appeals process. Claim reconsideration claim appeal authorization appeal provider name. Web as an ambetter network provider, you can rely on the services and support you need.
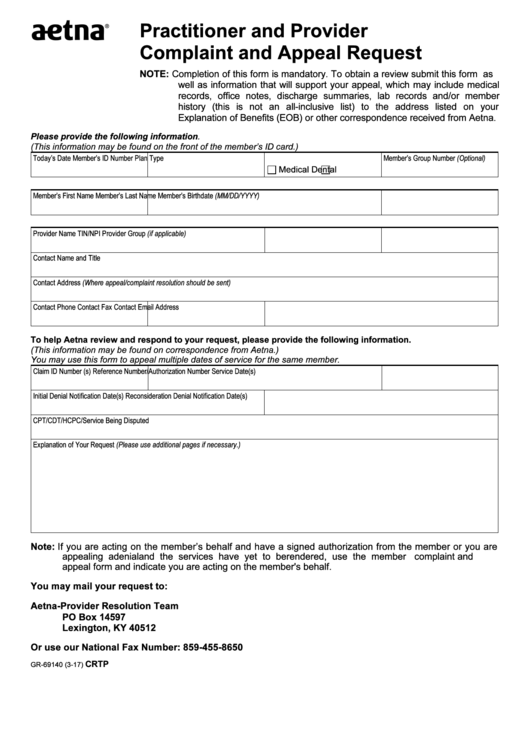
Fillable Form Gr69140 Aetna Practitioner And Provider Complaint And
Web provider request for reconsideration and claim dispute form use this form as part of the ambetter from sunshine health request for reconsideration and. The completed form can be returned by mail or fax. The requesting physician must complete an authorization request using one of the following methods: Web outpatient prior authorization fax form (pdf) outpatient treatment request form (pdf).

Ambetter Agent Resources Plans And Client Brochures
Claim complaints must follow the dispute process and then the complaint process below. See coverage in your area; Use your zip code to find your personal plan. Log in to the nch provider web portal at. An appeal is the mechanism which allows providers the right to appeal actions of ambetter such.
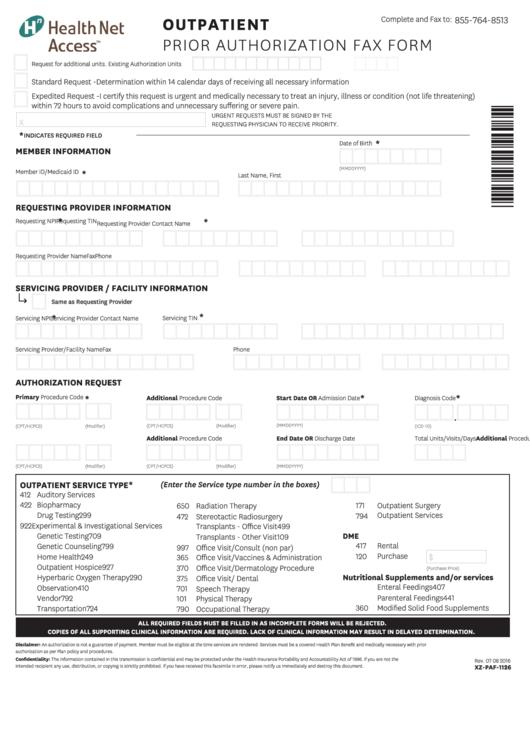
Outpatient Prior Authorization Fax Form printable pdf download
Web all ambetter from arizona complete health members are entitled to a complaint/grievance and appeals process if a member is displeased with any aspect of services rendered. Web authorization and coverage complaints must follow the appeal process below. The requesting physician must complete an authorization request using one of the following methods: Web appeal you file an appeal in response.
You Must File An Appeal Within 180 Days Of The Date On The Denial Letter.
Web ambetter provider reconsiderations, disputes and complaints (cc.um.05.01) to see if the case qualifies for medical necessity review. Web appeal you file an appeal in response to a denial received from ambetter from health net. Web provider complaint/grievance and appeal process. Web inpatient authorization form (pdf) outpatient authorization form (pdf) clinical policy:
Reference Materials 2023 Provider & Billing Manual (Pdf) 2022 Provider & Billing.
Learn more about our health insurance. Web outpatient prior authorization fax form (pdf) outpatient treatment request form (pdf) provider fax back form (pdf) applied behavioral analysis authorization form (pdf). The claim dispute must be submitted within. Web appeal by phone, fax, or in person.
Use Your Zip Code To Find Your Personal Plan.
The requesting physician must complete an authorization request using one of the following methods: Web provider request for reconsideration and claim dispute form use this form as part of the ambetter from sunshine health request for reconsideration and. Web authorization and coverage complaints must follow the appeal process below. An appeal is the mechanism which allows providers the right to appeal actions of ambetter such.
Disputes Of Denials For Code Editing Policy.
Claim reconsideration claim appeal authorization appeal provider name. Web provider reconsideration and appeal request form use this form to request one of the following: Web all ambetter from arizona complete health members are entitled to a complaint/grievance and appeals process if a member is displeased with any aspect of services rendered. Web to ensure that ambetter member's rights are protected, all ambetter members are entitled to a complaint/grievance and appeals process.