Dental Registration Form Pdf
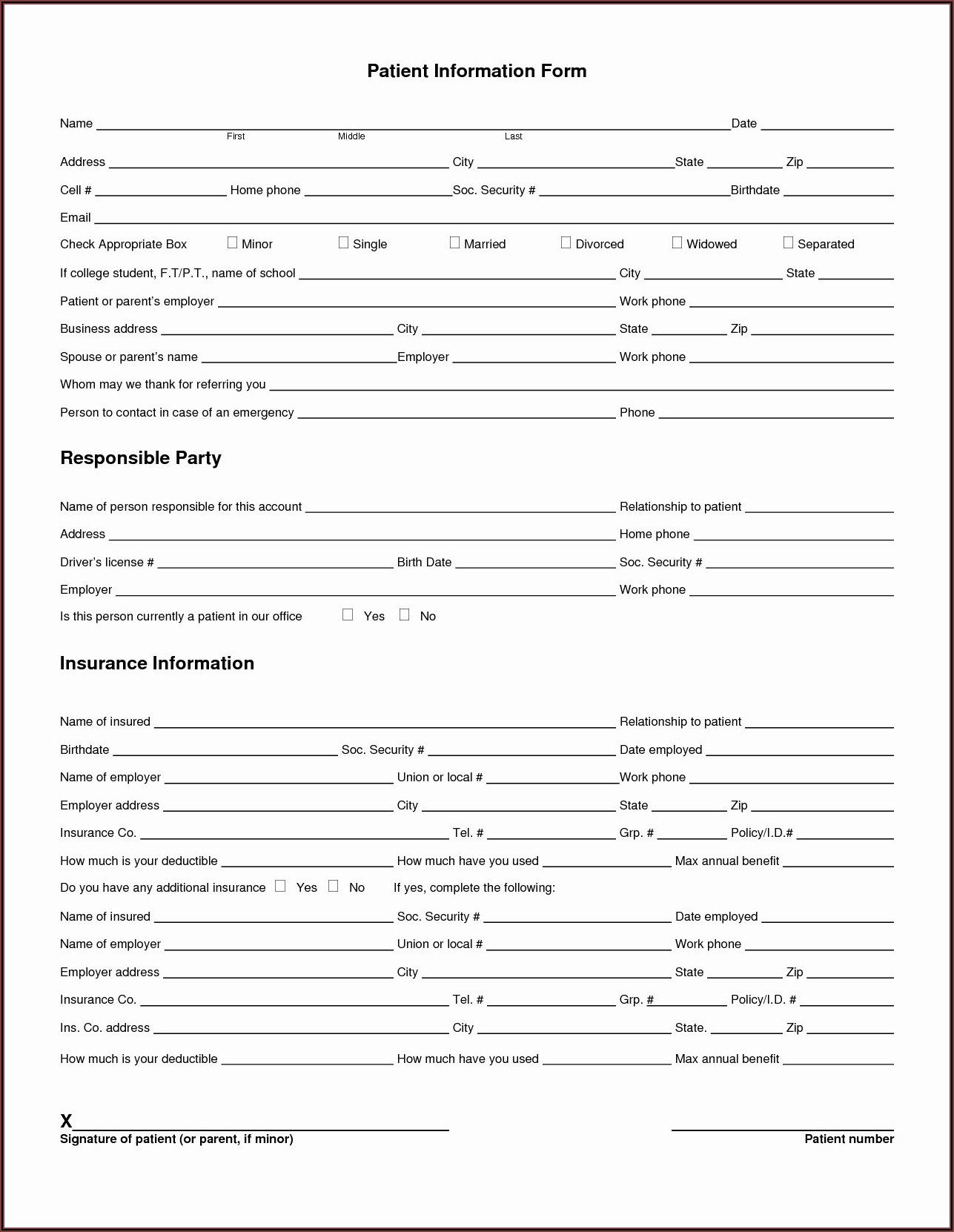
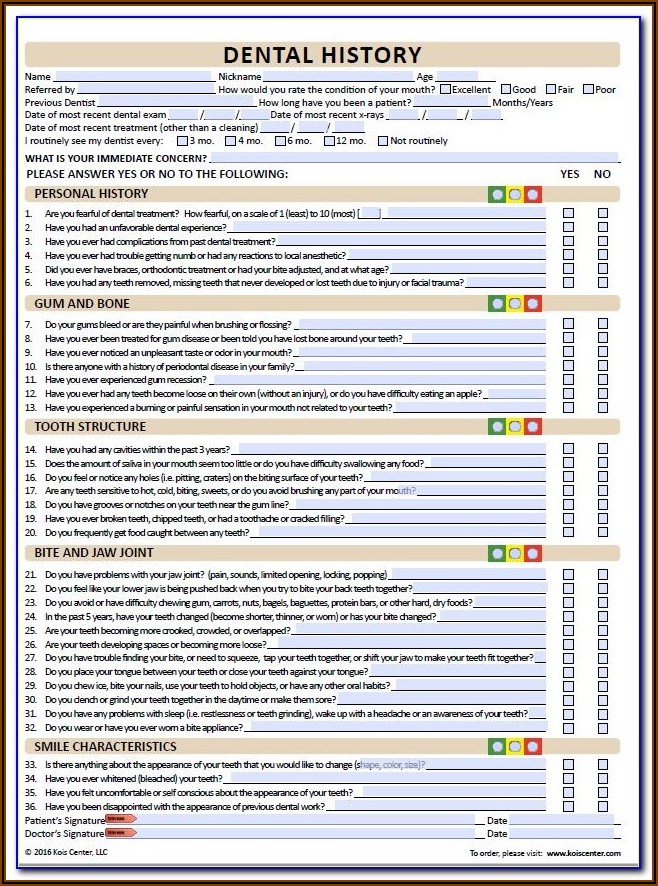
Dental Registration Form Pdf - This should contain the logo of the dental service. Web use the 2021 edition of the ada patient dental and medical health history information form to collect pertinent health information and history from your patients before. Web dental appointment policy in an effort to ensure access for all our dental patients. Web dental registration form ‐ adult updated 2/2018 patient information today’s date: Adhd cancer aids/hiv codeine allergy diabetes. Then read and sign the section at the bottom of form. Web dental treatment consent form please read and initial the items checked below. Web ada to offer new dental claim form in 2024. Web new patient registration form have you ever had any of the following? ___ / ___ / ______ last name first m.i.
Web creating a simple dental records release will be easily done with the help of the steps below: This material is educational only, does not constitute. Twenty four (24) to forty eight (48) hours before your. We want to deliver the same quality care in these. Web complete your patient forms in advance of your appointment. Single married divorced child other first name: This should contain the logo of the dental service. Then read and sign the section at the bottom of form. Web ada to offer new dental claim form in 2024. Patient registration form american dental association www.ada.org dental insurance information dental information for the following.
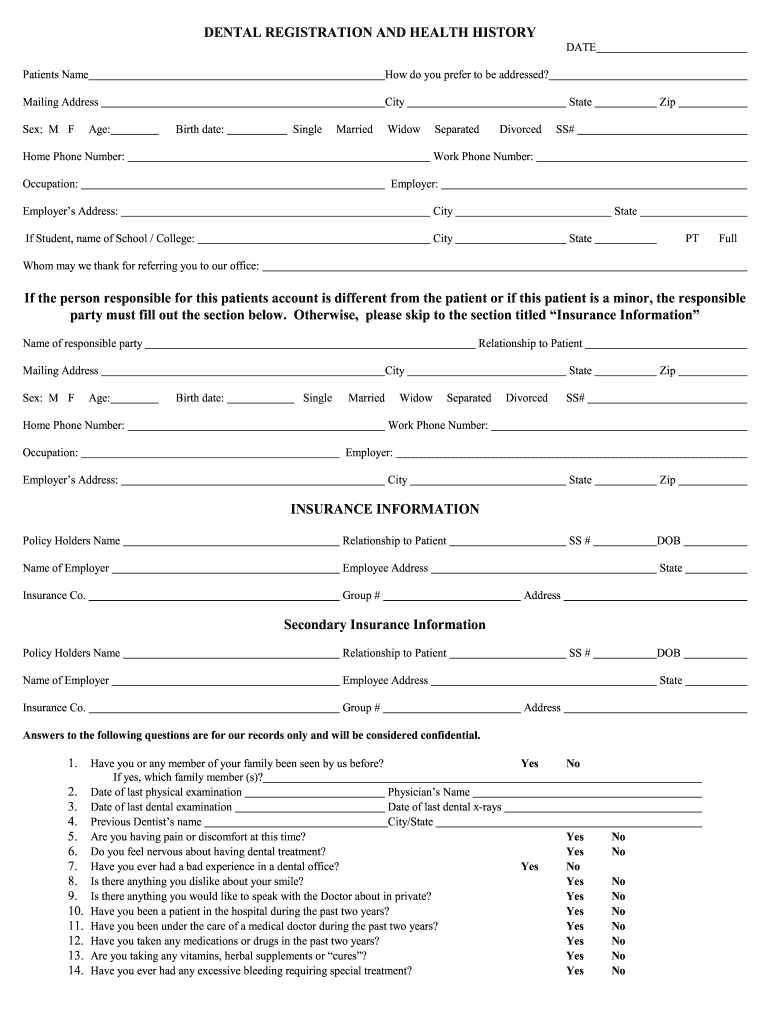
Web dental registration form ‐ adult updated 2/2018 patient information today’s date: Single married divorced child other first name: Kansas department for children and families. Web patient registration form today’s date: Central road, arlington heights, il 60005 ph: Payspan (pdf) secure portal (pdf) provider resource guide (pdf) outpatient. Web creating a simple dental records release will be easily done with the help of the steps below: Web ada to offer new dental claim form in 2024. Twenty four (24) to forty eight (48) hours before your. Please check those that apply:
Free Printable Dental Charting Forms Form Resume Examples Wk9y658AY3
University health 2301 holmes street kansas city, mo 64108 Please check those that apply: Great for dual and overlapping insurance policies within families, this printable medical coverage form concerns dental care. Single married divorced child other first name: Payspan (pdf) secure portal (pdf) provider resource guide (pdf) outpatient.
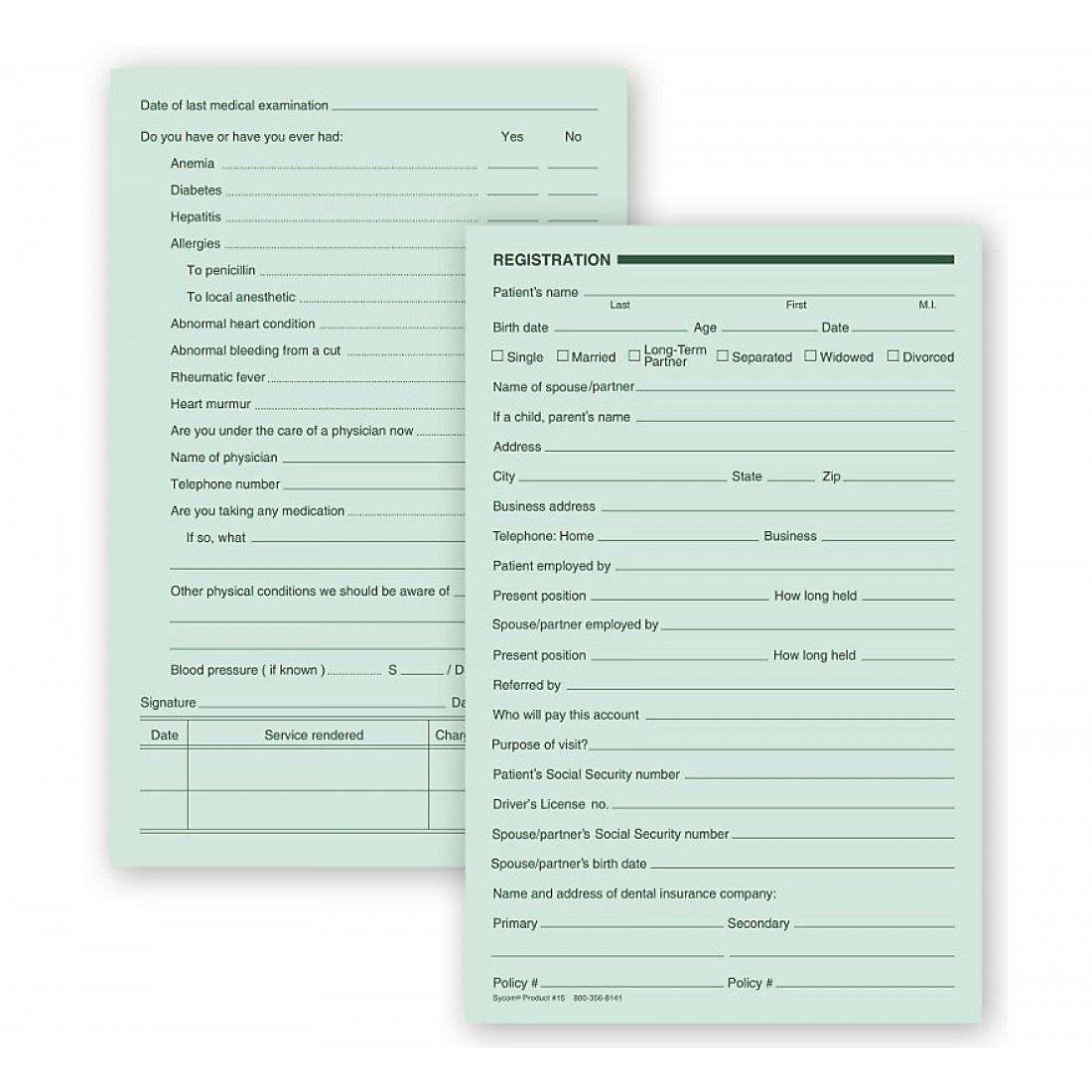
Dental Registration Forms Two Sided Green Ledger
Payspan (pdf) secure portal (pdf) provider resource guide (pdf) outpatient. Web patient registration form today’s date: Single married divorced child other first name: Web ada to offer new dental claim form in 2024. Web duplication or distribution by any other party requires the prior written approval of the american dental association.

Dental Patient Registration form Template Best Of Medical History form
Kansas department for children and families. Central road, arlington heights, il 60005 ph: Twenty four (24) to forty eight (48) hours before your. Web dental appointment policy in an effort to ensure access for all our dental patients. Adhd cancer aids/hiv codeine allergy diabetes.

28 New Patient Registration form Template in 2020 Registration form
Web duplication or distribution by any other party requires the prior written approval of the american dental association. Then read and sign the section at the bottom of form. Great for dual and overlapping insurance policies within families, this printable medical coverage form concerns dental care. Foster care licensing and division. Web dental registration form ‐ adult updated 2/2018 patient.
Dental Registration And History Form 20202021 Fill and Sign
This material is educational only, does not constitute. ___ / ___ / ______ last name first m.i. Foster care licensing and division. Web use the 2021 edition of the ada patient dental and medical health history information form to collect pertinent health information and history from your patients before. Kansas department for children and families.

Dental Patient Registration form Template Inspirational Best S Of
Great for dual and overlapping insurance policies within families, this printable medical coverage form concerns dental care. Please check those that apply: Web dental registration form ‐ adult updated 2/2018 patient information today’s date: Kansas department for children and families. Web patient registration form today’s date:
Free Dental Charting Forms Form Resume Examples AjYdX7qbYl
Web dental appointment policy in an effort to ensure access for all our dental patients. Foster care licensing and division. Learn more, plus see a sample form and completion instructions. Web duplication or distribution by any other party requires the prior written approval of the american dental association. Web use the 2021 edition of the ada patient dental and medical.
Dentist Registration Form Fill Online, Printable, Fillable, Blank
___ / ___ / ______ last name first m.i. Single married divorced child other first name: Web new patient registration form patient personal information title last, first address nickname city, state, zip email health care guardian name health care guardian. This material is educational only, does not constitute. We want to deliver the same quality care in these.
Free Patient Registration form Template Of New Patient Registration
Central road, arlington heights, il 60005 ph: Web creating a simple dental records release will be easily done with the help of the steps below: University health 2301 holmes street kansas city, mo 64108 This should contain the logo of the dental service. Web new patient registration form have you ever had any of the following?

Dental Patient Registration form Template Unique 27 Of Dental New
Web patient registration form today’s date: This should contain the logo of the dental service. You can also download it, export it or print it out. Then read and sign the section at the bottom of form. Web creating a simple dental records release will be easily done with the help of the steps below:
Single Married Divorced Child Other First Name:
Date of birth ___ / ___ / ______ social security. ___ / ___ / ______ last name first m.i. Patient registration form american dental association www.ada.org dental insurance information dental information for the following. Web dental treatment consent form please read and initial the items checked below.
University Health 2301 Holmes Street Kansas City, Mo 64108
Central road, arlington heights, il 60005 ph: Then read and sign the section at the bottom of form. Web new patient registration form patient personal information title last, first address nickname city, state, zip email health care guardian name health care guardian. Web dental registration form ‐ adult updated 2/2018 patient information today’s date:
Web Ada To Offer New Dental Claim Form In 2024.
Web dental appointment policy in an effort to ensure access for all our dental patients. Web new patient registration form have you ever had any of the following? This material is educational only, does not constitute. Twenty four (24) to forty eight (48) hours before your.
Adhd Cancer Aids/Hiv Codeine Allergy Diabetes.
You can also download it, export it or print it out. Web this document states the patient’s informed consent to allow the medical practitioners to administer the necessary medical treatment during an emergency when the patient is. Web complete your patient forms in advance of your appointment. Our patients' care needs are important for their overall health.