Form 1500 Printable
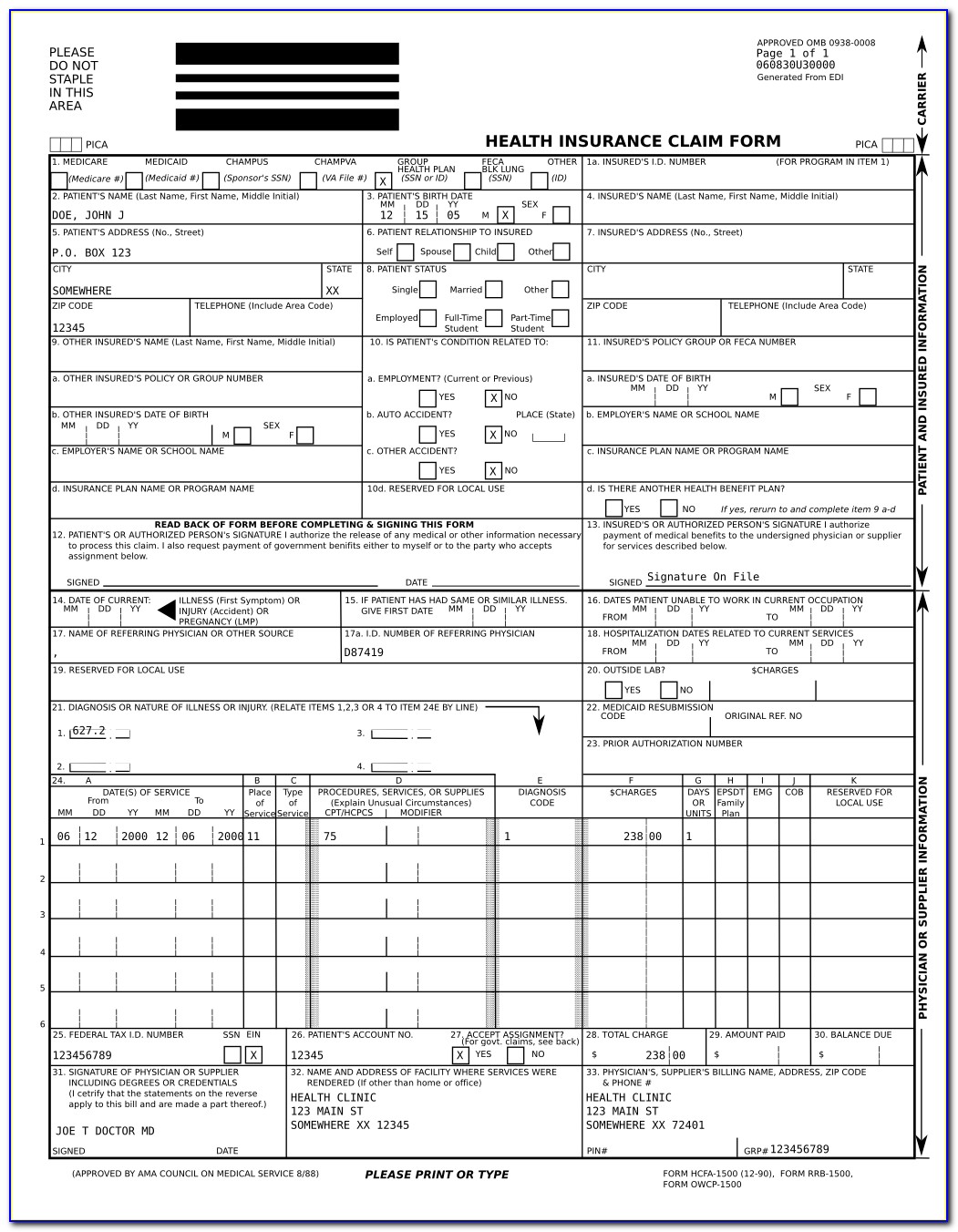
Form 1500 Printable - Any one who misrepresents or falsifies essential information to receive payment from federal funds requested by this form may upon conviction be subject to fine and imprisonment under applicable federal laws. Web no part b medicare benefits may be paid unless this form is received as required by existing law and regulations (42 cfr 424.32). Insured’s name (last name, first name, middle initial) 7. Read the instructions and tips below first. The nucc has developed this general instructions document for completing the 1500claim form. In addition to medicare parts a/b and for medicare. Insured’s address (no., street) city state zip code telephone (include area code) 11. Get everything done in minutes. It is used for health care claims. Number (for program in item 1) 4.
Any one who misrepresents or falsifies essential information to receive payment from federal funds requested by this form may upon conviction be subject to fine and imprisonment under applicable federal laws. Save or instantly send your ready documents. Number (for program in item 1) 4. If you are planning to ship something overseas, be sure to use usps form 1500. Keep pages 1 and 3 for your records. Web health insurance claim form 1500 printable. In addition to medicare parts a/b and for medicare. Read the instructions and tips below first. The nucc has developed this general instructions document for completing the 1500claim form. Web fillable cms claim form 1500.
Keep pages 1 and 3 for your records. Detailed information about the medical treatment will be required. Because this form is used by various government and private health programs, see separate instructions issued by applicable programs. The nucc has developed this general instructions document for completing the 1500claim form. Easily fill out pdf blank, edit, and sign them. Web health insurance claim form 1500 printable. This document is intended to be a guide for completing the 1500 claim form and not definitive instructions for this purpose. If you are planning to ship something overseas, be sure to use usps form 1500. Insured’s name (last name, first name, middle initial) 7. Our free fillable cms 1500 form pdf is a resource you can keep on hand for repeated use.
Free Health Insurance Claim form 1500 Template Of Medical Claim form
This form allows you to declare the contents of your package, as well as its value. Because this form is used by various government and private health programs, see separate instructions issued by applicable programs. Our free fillable cms 1500 form pdf is a resource you can keep on hand for repeated use. Web health insurance claim form 1500 printable..
Printable Hcfa 1500 Claim Form Form Resume Examples pv9wXnJxY7
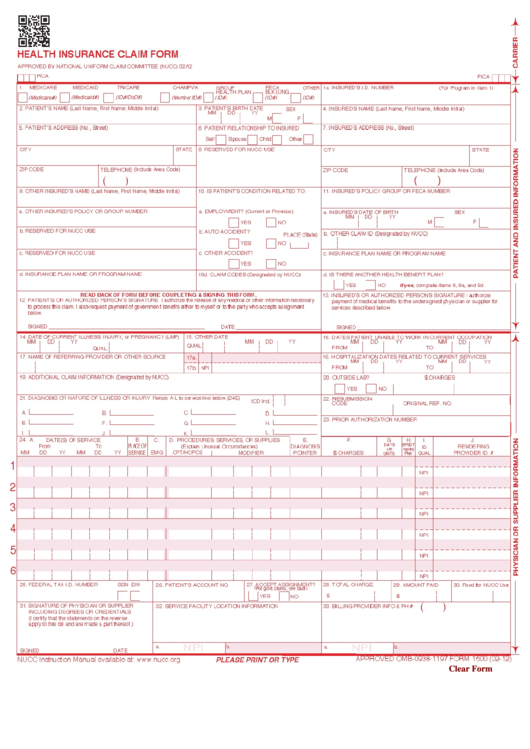
Web a hcfa 1500 form is used by the health care financing administration. 3.50 out of 5) download cms claim form 1500 which is used by health care professionals to bill medicare and medicaid. Easily fill out pdf blank, edit, and sign them. Read the instructions and tips below first. Web cms 1500 dynamic list information.

Cms 1500 Form Printable Form Resume Examples kDp3Oxr80Q
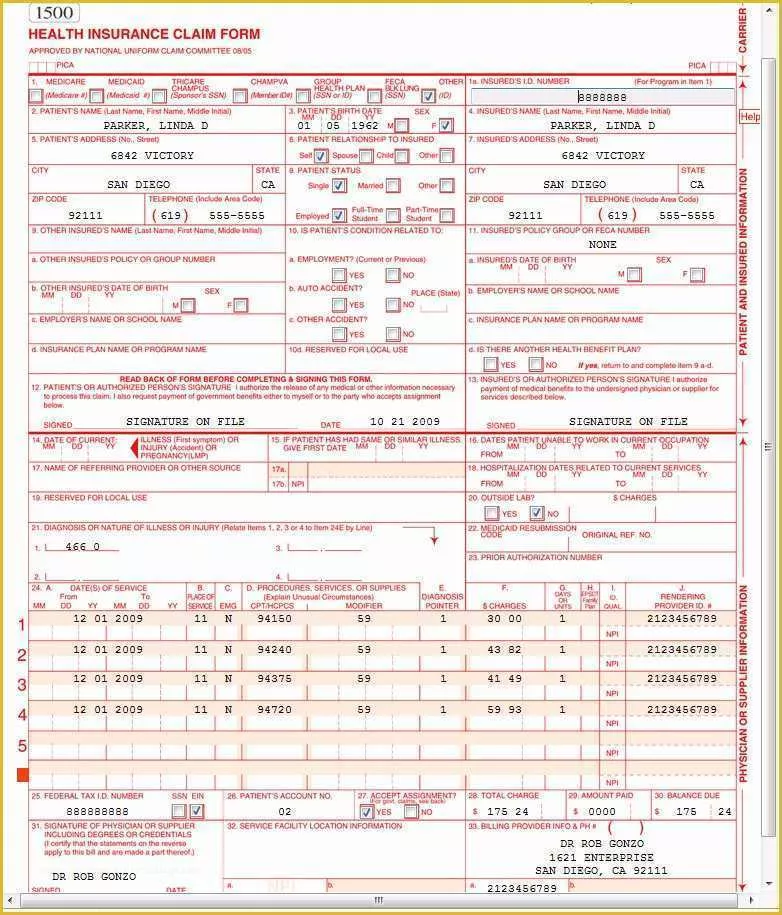
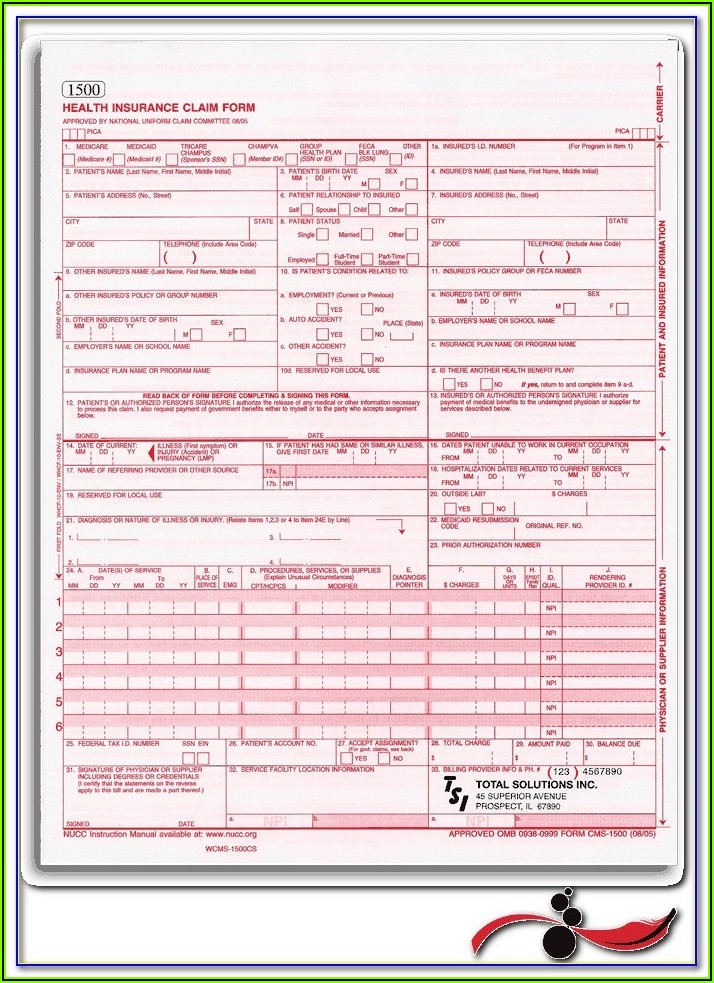
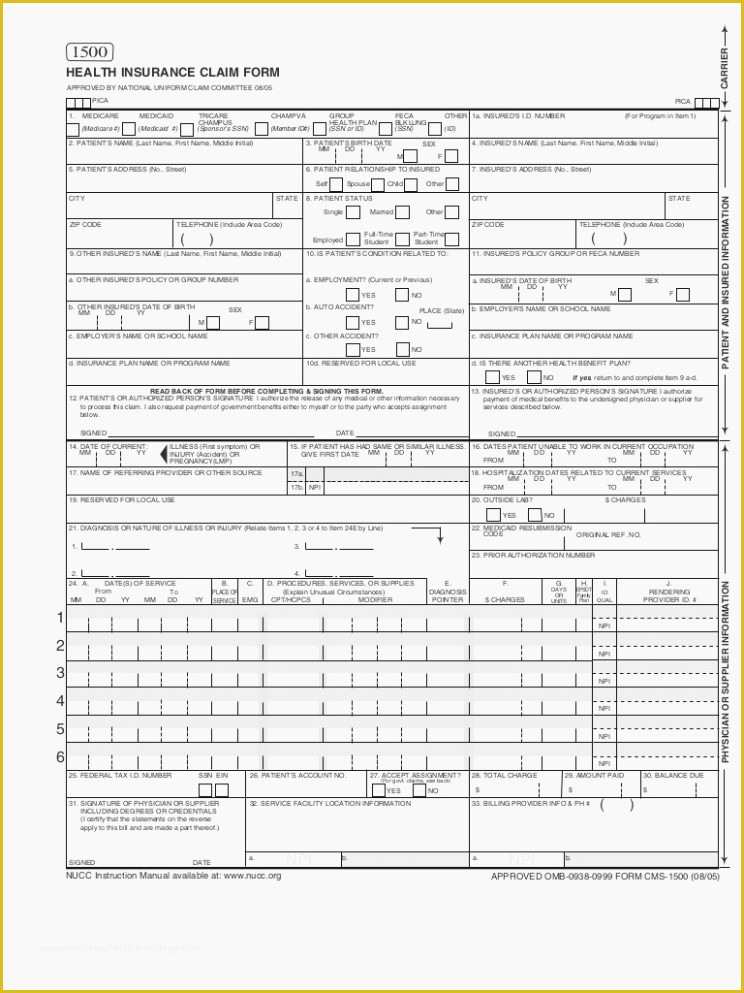
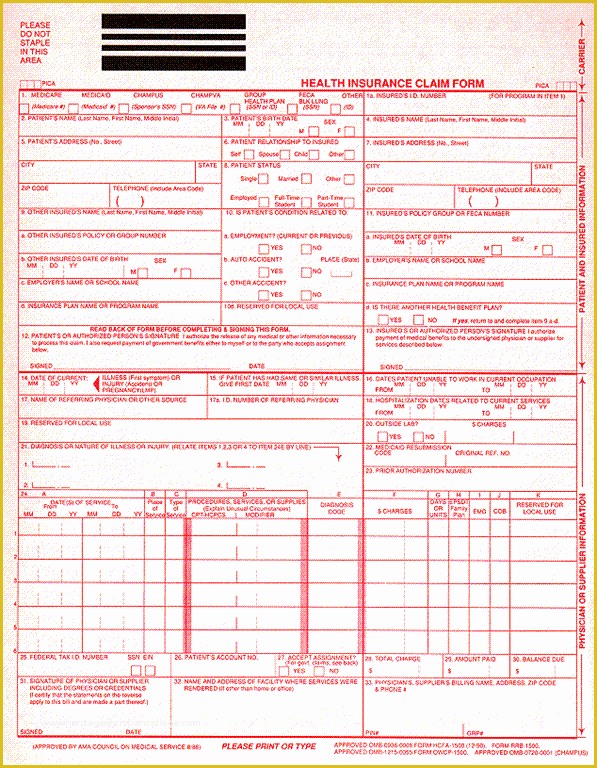
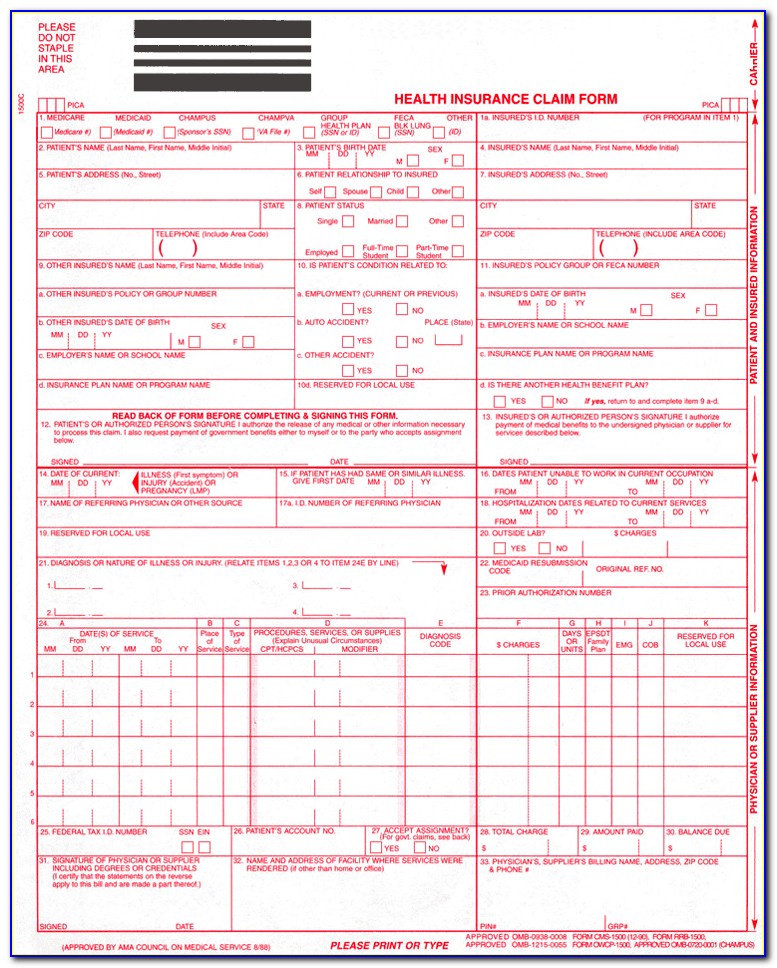
Simply click on the appropriate form and print it using the [print] button provided near the top of the form. Web reset form print form 1500 health insurance claim form approved by national uniform claim committee 08/05. Check out how easy it is to complete and esign documents online using fillable templates and a powerful editor. Or • the government.
Fillable Form 1500 Health Insurance Claim Form printable pdf download
Web reset form print form 1500 health insurance claim form approved by national uniform claim committee 08/05. Show details how it works open the usps resignation form and follow the instructions easily sign the usps form 1094 pdf with your finger To print cms 1500 claim form, you will need a copy of adobe acrobat reader, which you can download.
Free Cms 1500 Template for Word Of 1500 Claim form Pdf Hcfa 1500 form
Our free fillable cms 1500 form pdf is a resource you can keep on hand for repeated use. Sign up to get the latest information about your choice of cms topics. Web reset form print form 1500 health insurance claim form approved by national uniform claim committee 08/05. Fill out the health insurance claim form online and print it out.
Free Health Insurance Claim form 1500 Template Of Medical Claim form
Number (for program in item 1) 4. Insured's name (last name, first name, middle initial) 7. If you are planning to ship something overseas, be sure to use usps form 1500. Because this form is used by various government and private health programs, see separate instructions issued by applicable programs. Any one who misrepresents or falsifies essential information to receive.
Blank Fillable Cms 1500 Form Form Resume Examples o85pdJY5ZJ
The nucc has developed this general instructions document for completing the 1500claim form. Insured's name (last name, first name, middle initial) 7. Insured’s address (no., street) city state zip code telephone (include area code) 11. Department of health & human services. Web • tfp data systems:

Hcfa 1500 Form Pdf Form Resume Examples
Web complete health claim form 1500 online with us legal forms. Our free fillable cms 1500 form pdf is a resource you can keep on hand for repeated use. Detailed information about the medical treatment will be required. Web sign and date the application in the authorization section and submit it to any post office. Web cms 1500 dynamic list.

Medicare Form 1500 Instructions Form Resume Examples QJ9el08B2m
Department of health & human services. Sign up to get the latest information about your choice of cms topics. Web fillable cms claim form 1500. Web no part b medicare benefits may be paid unless this form is received as required by existing law and regulations (42 cfr 424.32). This could be through medicare, champus, group health care, or other.
Cms 1500 Claim Form Fillable Download Free Form Resume Examples
Because this form is used by various government and private health programs, see separate instructions issued by applicable programs. When your application has been processed, we will send you information about the effective date of your listing and the procedure for reporting a violation of your protected status. Fill out the health insurance claim form online and print it out.
Web One Popular Form Is Usps Form 1500, Which Is Used For International Shipments.
Because this form is used by various government and private health programs, see separate instructions issued by applicable programs. Read the instructions and tips below first. Insured’s address (no., street) city state zip code telephone (include area code) 11. Web fillable cms claim form 1500.
It Is Used To Submit A Bill Or Charge For Health Insurance Coverage.
The form helps organize the mailings and ensure that all pieces are correctly addressed and delivered. Check out how easy it is to complete and esign documents online using fillable templates and a powerful editor. The usps form 1500 is an essential form for businesses and organizations mailing large quantities of mail. It is used for health care claims.
Web Cms 1500 Dynamic List Information.
This could be through medicare, champus, group health care, or other forms of insurance. Keep pages 1 and 3 for your records. In addition to medicare parts a/b and for medicare. Insured's name (last name, first name, middle initial) 7.
You Can Decide How Often To.
Web complete health claim form 1500 online with us legal forms. Insured’s name (last name, first name, middle initial) 7. Fill out the health insurance claim form online and print it out for free. Number (for program in item 1) 4.