How To Fill Out Hipaa Form
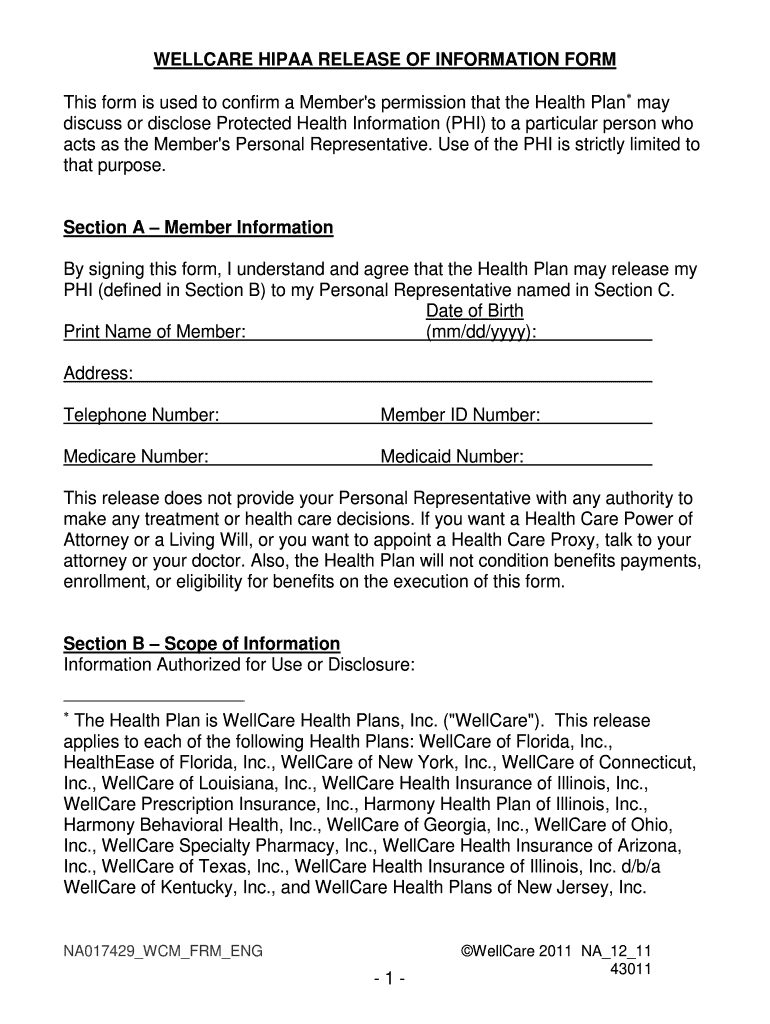
How To Fill Out Hipaa Form - Web the forms provided here represent only a few of the new administrative measures hipaa will require. Granting access to your medical records 4 min read last reviewed or updated. Web one authorization form may be used to authorize uses and disclosures by classes or categories of persons or entities, without naming the particular persons or entities. This form is to be used by a patient or legal representative to authorize the release of information to a third party (other than a family member or friend) such as an. Fill in your name in the line titled “individual’s name” and your social security. Find translations of health insurance portability. Web a hipaa authorization form gives covered entities permission to use protected health information for purposes other than treatment, payment, or health care operations. Web why do i need a hipaa consent form? Web up to 24% cash back ⌃ medical records and insurance claims hipaa authorization: Open and fill out the health information privacy complaint form package in.
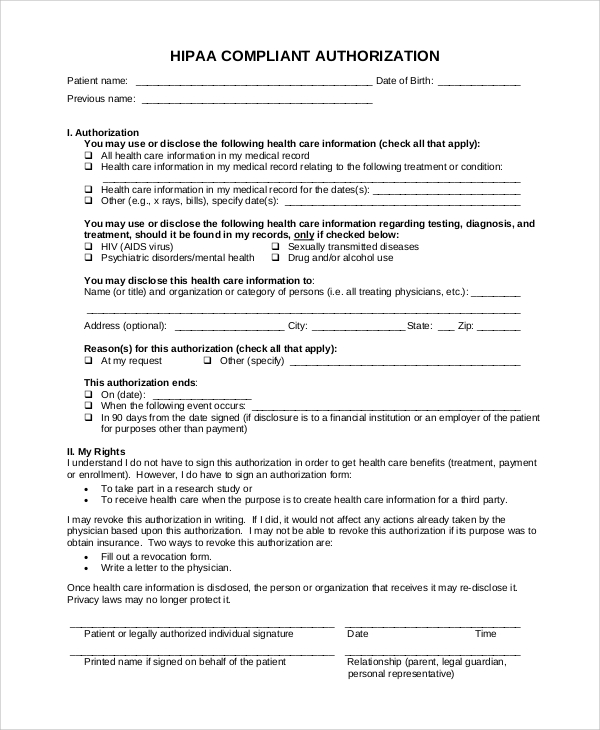
Web if you believe your rights are being denied or your health information isn’t being protected, you can. File a complaint with your provider or health insurer. Web please follow these instructions in filling out the authorization for disclosure of phi form: Ad privacy auth form, subscribe now. Ad answer simple questions to make a hipaa authorization form on any device in minutes. Web one authorization form may be used to authorize uses and disclosures by classes or categories of persons or entities, without naming the particular persons or entities. We may reach out for you to provide additional documentation if needed. Web authorization for release of health information pursuant to hipaa [this form has been approved by the new york state department of health] patient. Web in section 1 insert the name of health care provider (hospital, physician, practice, etc.) you are authorizing to release your information (most often this will be our practice name),. Web what is the full form of hipaa in the united states?
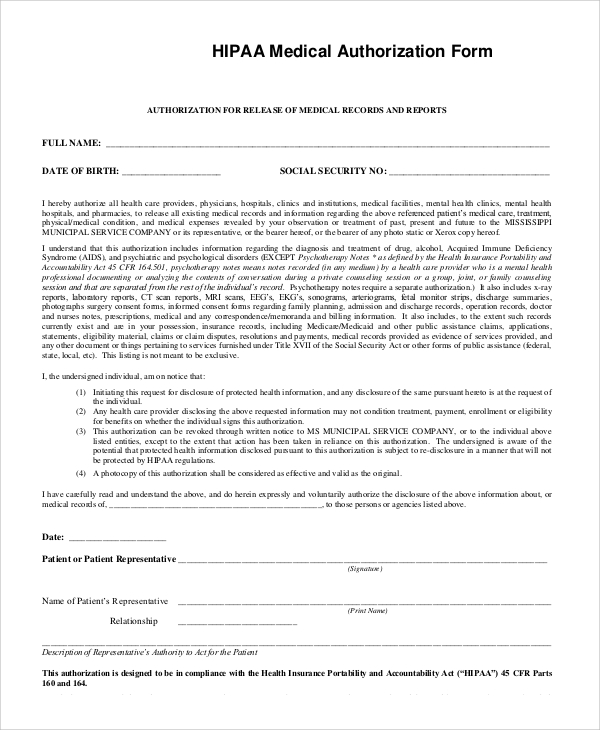
Fill in your name in the line titled “individual’s name” and your social security. File a complaint with your provider or health insurer. Web 7) sign the form 8) if you are a personal representative, print your name and relationship. Upload, modify or create forms. Web up to 24% cash back ⌃ medical records and insurance claims hipaa authorization: Web one authorization form may be used to authorize uses and disclosures by classes or categories of persons or entities, without naming the particular persons or entities. Open and fill out the health information privacy complaint form package in. This form is to be used by a patient or legal representative to authorize the release of information to a third party (other than a family member or friend) such as an. Easily customize your hipaa authorization form. Web a hipaa authorization form gives covered entities permission to use protected health information for purposes other than treatment, payment, or health care operations.

HIPAA Compliance Agreement Fill and Sign Printable Template Online
Web 7) sign the form 8) if you are a personal representative, print your name and relationship. Web in section 1 insert the name of health care provider (hospital, physician, practice, etc.) you are authorizing to release your information (most often this will be our practice name),. We may reach out for you to provide additional documentation if needed. Web.
Sample Hipaa Authorization Form The Document Template
Web a hipaa (health insurance portability and accountability act) release allows physicians to share information and medical records with you, and a medical power of. Web file a complaint using the health information privacy complaint form package. Try it for free now! Web a hipaa authorization form gives covered entities permission to use protected health information for purposes other than.

How to fill out HIPAA form YouTube
Web why do i need a hipaa consent form? Fill in your name in the line titled “individual’s name” and your social security. Web file a complaint using the health information privacy complaint form package. We may reach out for you to provide additional documentation if needed. File a complaint with your provider or health insurer.
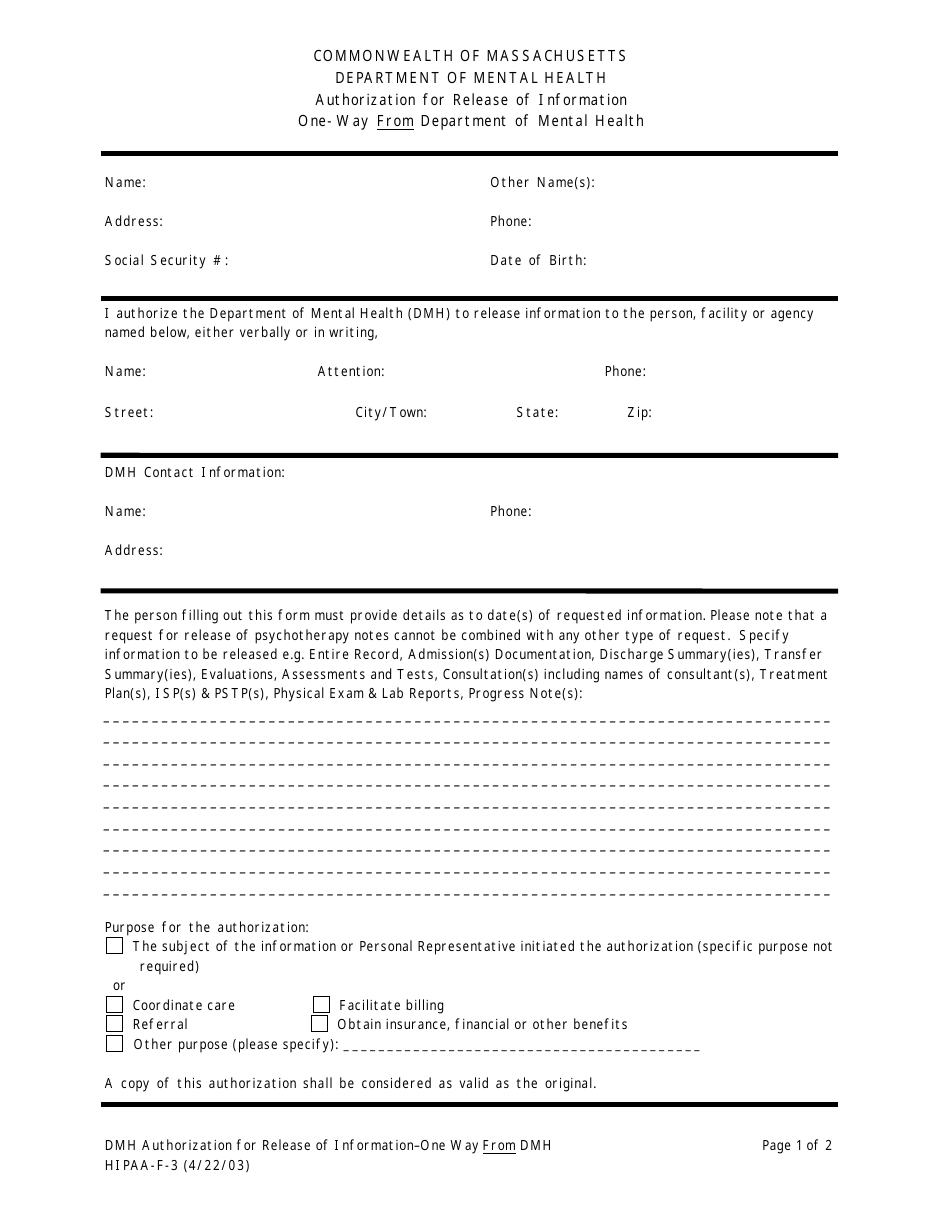
Form HIPAAF3 Download Printable PDF or Fill Online Authorization for
Granting access to your medical records 4 min read last reviewed or updated. Easily customize your hipaa authorization form. Try it for free now! Fill in your name in the line titled “individual’s name” and your social security. Web a hipaa (health insurance portability and accountability act) release allows physicians to share information and medical records with you, and a.

HIPAA Form Fill Out and Sign Printable PDF Template signNow
We may reach out for you to provide additional documentation if needed. Web why do i need a hipaa consent form? Web up to 24% cash back ⌃ medical records and insurance claims hipaa authorization: Web the forms provided here represent only a few of the new administrative measures hipaa will require. Try it for free now!

PA HIPAA Authorization Form for Release of Medical Record Information
Web one authorization form may be used to authorize uses and disclosures by classes or categories of persons or entities, without naming the particular persons or entities. File a complaint with your provider or health insurer. Web the forms provided here represent only a few of the new administrative measures hipaa will require. Open and fill out the health information.

Hipaa Release Form Wisconsin 20202021 Fill and Sign Printable
Web 7) sign the form 8) if you are a personal representative, print your name and relationship. Web if you believe your rights are being denied or your health information isn’t being protected, you can. Web up to 24% cash back ⌃ medical records and insurance claims hipaa authorization: There are other forms, (e.g., a business associate agreement) and more..
Hipaa Release Form 20202022 Fill and Sign Printable Template Online
Health insurance portability and accountability act of 1996. Easily customize your hipaa authorization form. Web if you believe your rights are being denied or your health information isn’t being protected, you can. Web a hipaa (health insurance portability and accountability act) release allows physicians to share information and medical records with you, and a medical power of. Web up to.
FREE 9+ Sample Hipaa Forms in PDF MS Word
Web if you believe your rights are being denied or your health information isn’t being protected, you can. File a complaint with your provider or health insurer. Web why do i need a hipaa consent form? Web file a complaint using the health information privacy complaint form package. Upload, modify or create forms.
FREE 9+ Sample Hipaa Forms in PDF MS Word
Web in section 1 insert the name of health care provider (hospital, physician, practice, etc.) you are authorizing to release your information (most often this will be our practice name),. Health insurance portability and accountability act of 1996. Web file a complaint using the health information privacy complaint form package. Try it for free now! File a complaint with your.
Web 7) Sign The Form 8) If You Are A Personal Representative, Print Your Name And Relationship.
Web the forms provided here represent only a few of the new administrative measures hipaa will require. Web what is the full form of hipaa in the united states? There are other forms, (e.g., a business associate agreement) and more. Web why do i need a hipaa consent form?
Ad Privacy Auth Form, Subscribe Now.
Granting access to your medical records 4 min read last reviewed or updated. Find translations of health insurance portability. File a complaint with your provider or health insurer. Easily customize your hipaa authorization form.
We May Reach Out For You To Provide Additional Documentation If Needed.
Upload, modify or create forms. Web file a complaint using the health information privacy complaint form package. Web please follow these instructions in filling out the authorization for disclosure of phi form: Health insurance portability and accountability act of 1996.
Fill In Your Name In The Line Titled “Individual’s Name” And Your Social Security.
Ad answer simple questions to make a hipaa authorization form on any device in minutes. Web in section 1 insert the name of health care provider (hospital, physician, practice, etc.) you are authorizing to release your information (most often this will be our practice name),. Try it for free now! Web a hipaa (health insurance portability and accountability act) release allows physicians to share information and medical records with you, and a medical power of.