Medical Refusal Of Treatment Form
Medical Refusal Of Treatment Form - Ad pdffiller allows users to edit, sign, fill and share all type of documents online. Web refusal to permit medical treatment my doctor (physician name) has advised the following medical treatment: , my doctor has informed me of the following: The risks and complications of this medical treatment. The expected benefits of this medical treatment. Web refusal of care against medical advice criteria for refusing care the patient meets all of the following: Edit pdfs, create forms, collect data, collaborate with your team, secure docs and more. Web an advance decision (sometimes known as an advance decision to refuse treatment, an adrt, or a living will) is a decision you can make now to refuse a specific type of treatment at some time in the future. Evaluation please circle the following that apply: Choose the fillable fields and include.
Choose the fillable fields and include. The nature and advisability of this medical treatment. Open the document in our online editor. Is a patient over the age of 18 yrs. The expected benefits of this medical treatment. Web refusal of medical treatment for a work related injury have been advised to seek and understand that medical attention is available for my work related injury from my supervisor. Read the guidelines to find out which data you will need to give. Find the form you want in the library of templates. Evaluation please circle the following that apply: I understand that i may seek medical attention at a later time if deemed.
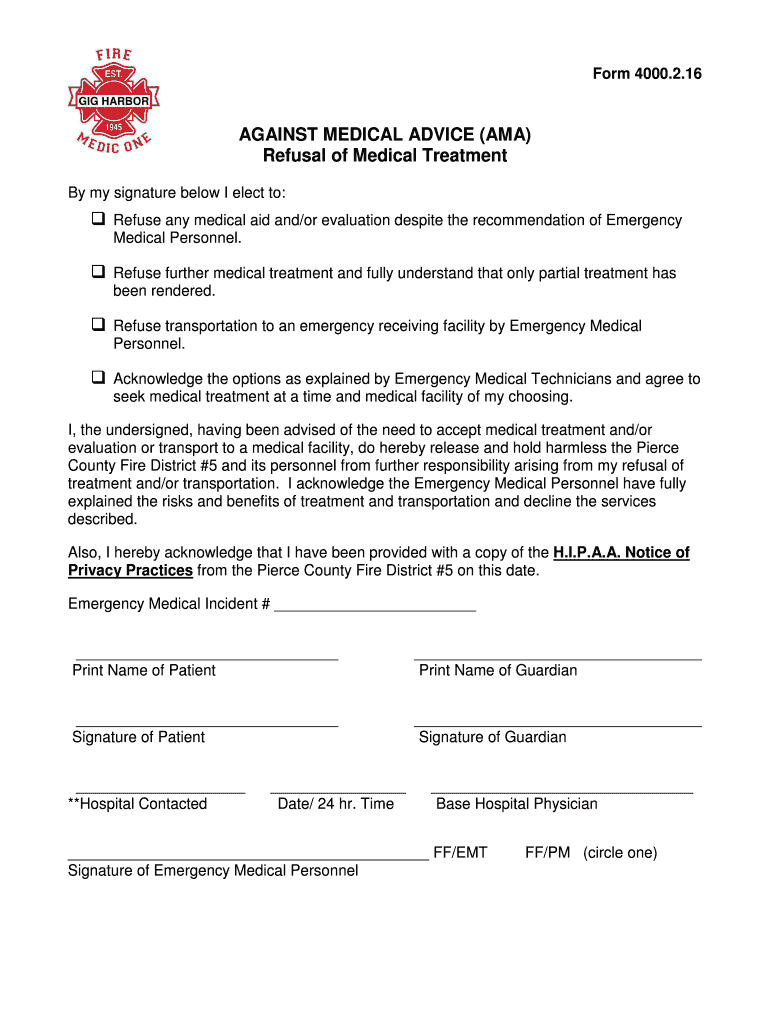
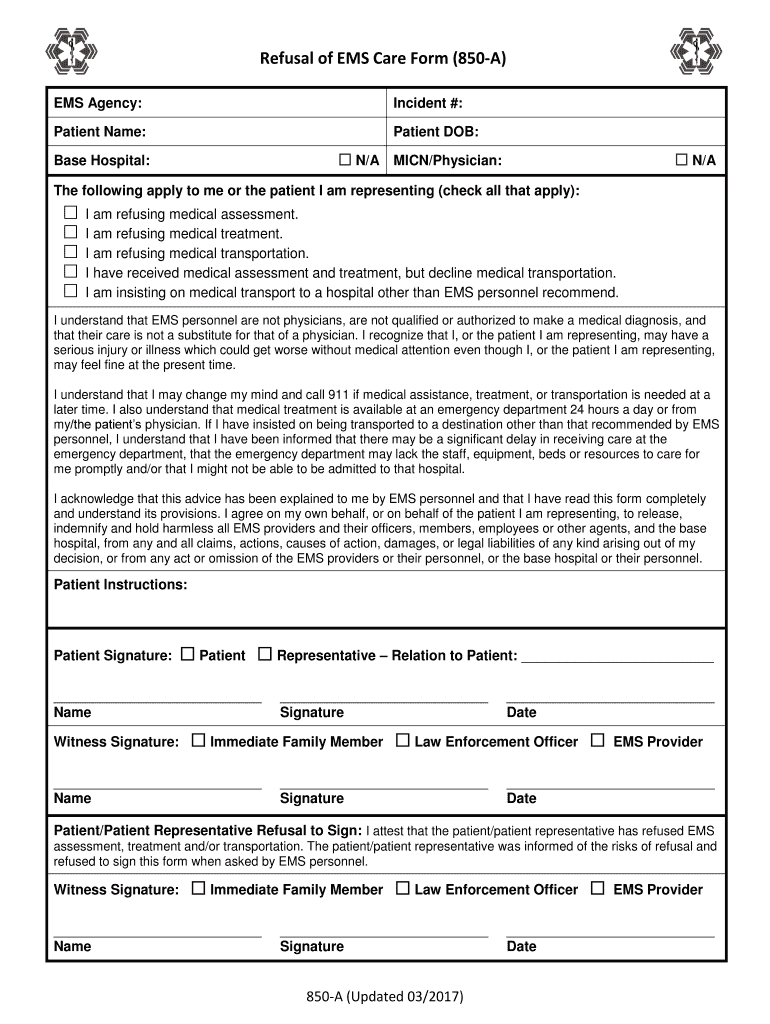
Web by signing below, you are acknowledging that ems personnel have advised you, and that you understand, the potential harm to your health that may result from your refusal of the recommended care; The nature and advisability of this medical treatment. And, you release ems and supporting personnel from liability resulting from refusal. Find the form you want in the library of templates. Description of injury [body part(s) injured]: Evaluation please circle the following that apply: Brief narrative description of the incident: Ad pdffiller allows users to edit, sign, fill and share all type of documents online. I understand that i may seek medical attention at a later time if deemed. Is a patient over the age of 18 yrs.
Ama Refusal Of Treatment Form Fill Out and Sign Printable PDF
The expected benefits of this medical treatment. Web by signing below, you are acknowledging that ems personnel have advised you, and that you understand, the potential harm to your health that may result from your refusal of the recommended care; Find the form you want in the library of templates. It lets your family, carers and health professionals know your.
Printable Refusal Of Medical Treatment Form
I am hereby declining to go to the clinic and/or doctor as advised by my supervisor. Web by signing below, you are acknowledging that ems personnel have advised you, and that you understand, the potential harm to your health that may result from your refusal of the recommended care; It lets your family, carers and health professionals know your wishes.

The Law and Paramedics (Ethics and Law in EMS) Part 3
Edit pdfs, create forms, collect data, collaborate with your team, secure docs and more. Web by signing below, you are acknowledging that ems personnel have advised you, and that you understand, the potential harm to your health that may result from your refusal of the recommended care; It lets your family, carers and health professionals know your wishes about refusing.

Medical Treatment Refusal Form Template amulette
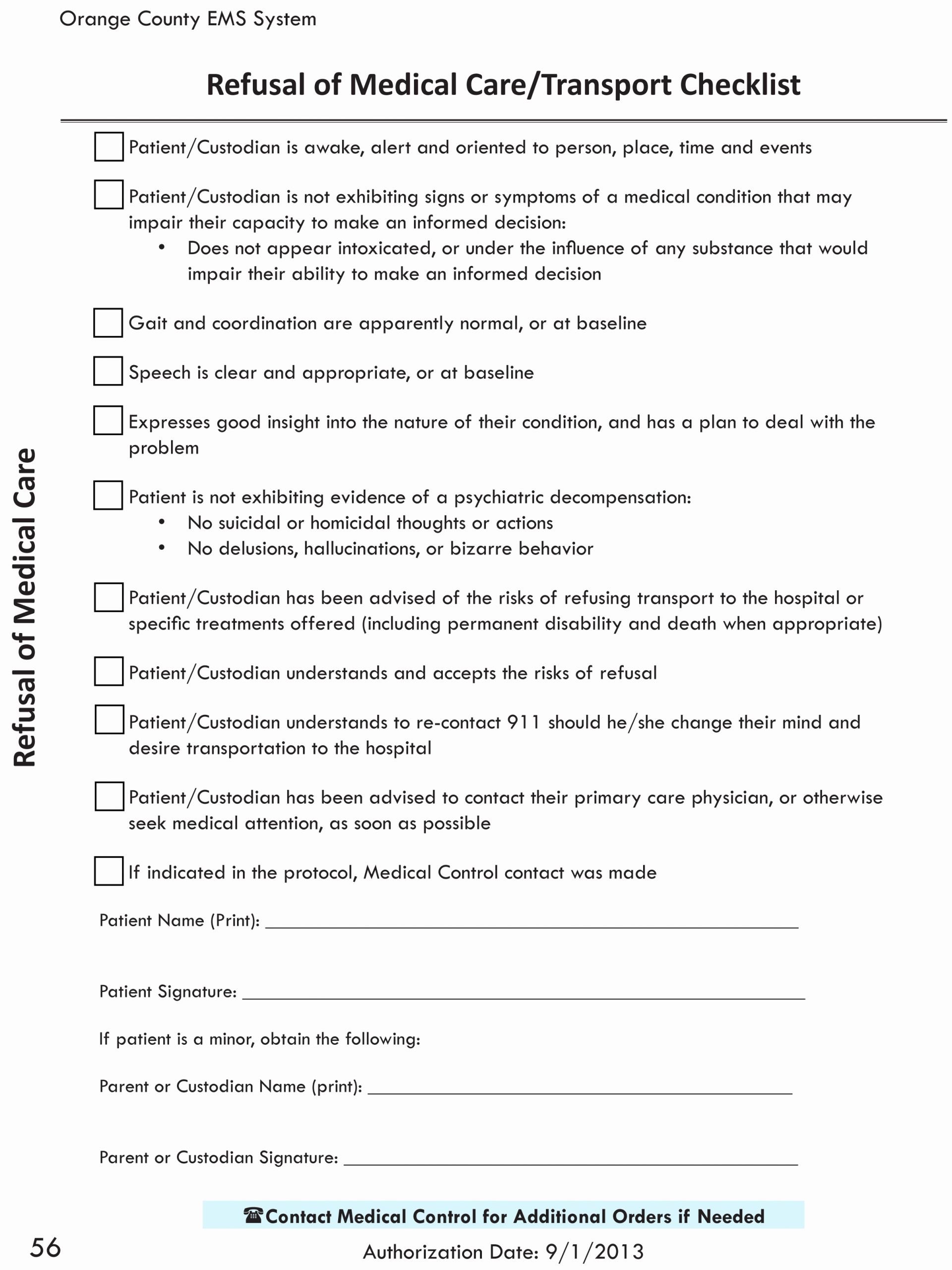
I understand that i may seek medical attention at a later time if deemed. Find the form you want in the library of templates. Choose the fillable fields and include. Altered level of consciousness alcohol or drug ingestion that would impair judgment Brief narrative description of the incident:
√ 20 Refusal Of Treatment form Sample ™ Dannybarrantes Template
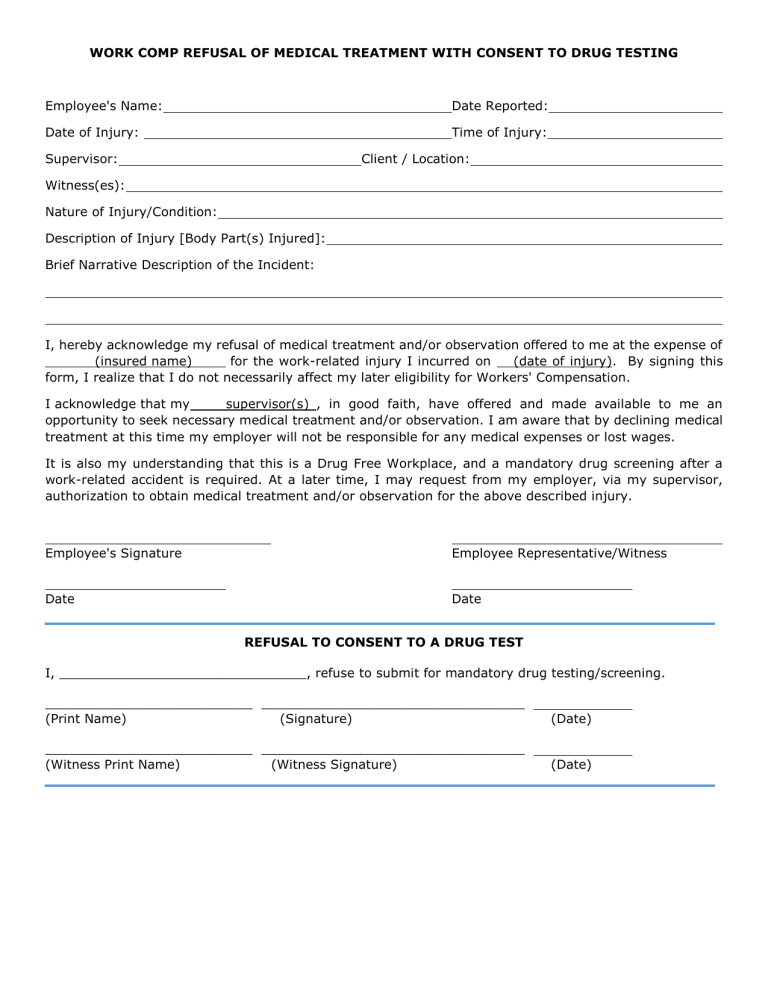
Web employee refusal of medical treatment form have been advised by my supervisor/safety specialist that i may seek medical treatment for the injury that may have occurred on the job per the below listed information. The nature and advisability of this medical treatment. Web an advance decision (sometimes known as an advance decision to refuse treatment, an adrt, or a.
Top 10 Refusal Of Medical Treatment Form Templates free to download in
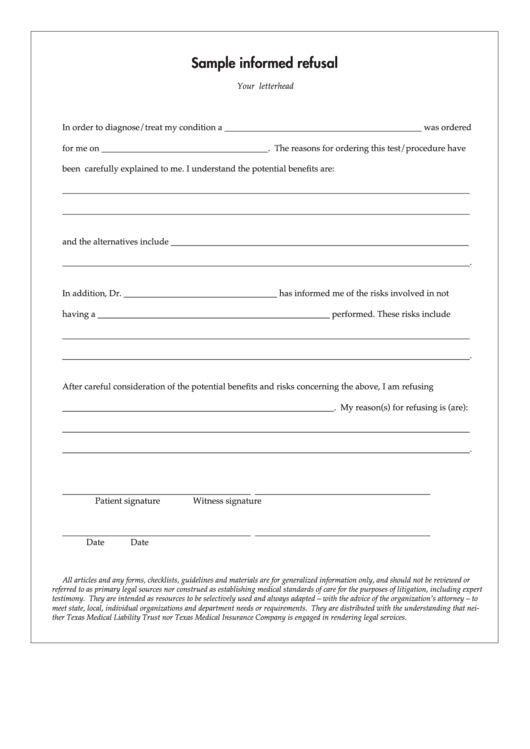
Web sample refusal of treatment i, _______________, refuse to consent to the following treatment/procedure/ diagnostic test/medication/referral as recommended by my physician, _______________ m.d./d.o.: The risks and complications of this medical treatment. Web an advance decision (sometimes known as an advance decision to refuse treatment, an adrt, or a living will) is a decision you can make now to refuse a.
Refusal of Medical Treatment or Observation
I understand that i may seek medical attention at a later time if deemed. The risks and complications of this medical treatment. Edit pdfs, create forms, collect data, collaborate with your team, secure docs and more. Choose the fillable fields and include. Web refusal of medical treatment for a work related injury have been advised to seek and understand that.
Top 10 Refusal Of Medical Treatment Form Templates free to download in
, my doctor has informed me of the following: It lets your family, carers and health professionals know your wishes about refusing treatment if you're unable to make or communicate. Edit pdfs, create forms, collect data, collaborate with your team, secure docs and more. I am hereby declining to go to the clinic and/or doctor as advised by my supervisor..
SSV EMS Agency Form 850A 20172021 Fill and Sign Printable Template
Find the form you want in the library of templates. The nature and advisability of this medical treatment. Web by signing below, you are acknowledging that ems personnel have advised you, and that you understand, the potential harm to your health that may result from your refusal of the recommended care; Web refusal of care against medical advice criteria for.

Refusal Of Medical Treatment Form California 20202022 Fill and Sign
, my doctor has informed me of the following: Brief narrative description of the incident: Web by signing below, you are acknowledging that ems personnel have advised you, and that you understand, the potential harm to your health that may result from your refusal of the recommended care; Web sample refusal of treatment i, _______________, refuse to consent to the.
The Nature And Advisability Of This Medical Treatment.
Web an advance decision (sometimes known as an advance decision to refuse treatment, an adrt, or a living will) is a decision you can make now to refuse a specific type of treatment at some time in the future. Web refusal of medical treatment for a work related injury have been advised to seek and understand that medical attention is available for my work related injury from my supervisor. Edit pdfs, create forms, collect data, collaborate with your team, secure docs and more. I am hereby declining to go to the clinic and/or doctor as advised by my supervisor.
Evaluation Please Circle The Following That Apply:
, my doctor has informed me of the following: Open the document in our online editor. Web refusal to permit medical treatment my doctor (physician name) has advised the following medical treatment: The expected benefits of this medical treatment.
It Lets Your Family, Carers And Health Professionals Know Your Wishes About Refusing Treatment If You're Unable To Make Or Communicate.
Ad pdffiller allows users to edit, sign, fill and share all type of documents online. Is a patient over the age of 18 yrs. Web employee refusal of medical treatment form have been advised by my supervisor/safety specialist that i may seek medical treatment for the injury that may have occurred on the job per the below listed information. Altered level of consciousness alcohol or drug ingestion that would impair judgment
I Understand That I May Seek Medical Attention At A Later Time If Deemed.
Web sample refusal of treatment i, _______________, refuse to consent to the following treatment/procedure/ diagnostic test/medication/referral as recommended by my physician, _______________ m.d./d.o.: Web by signing below, you are acknowledging that ems personnel have advised you, and that you understand, the potential harm to your health that may result from your refusal of the recommended care; Read the guidelines to find out which data you will need to give. Description of injury [body part(s) injured]: