Medical Release Form Ohio
Medical Release Form Ohio - That treatment from or payment of my claim will not to be impacted by. Web a catalog of ohio department of health program forms. Entry authorizing release of medical records and medical billing records; Application to release medical records and medical billing records; Do not alter this form. Tailored to fit your unique situation. There are three ways to request information from your medical record regarding your care at ohio state. While this form was developed by odm, this form can be used in any situation that needs a hipaa or 42 c.f.r. Web ohio provides compassionate release through judicial release1 and release as if on parole2 to eligible incarcerated individuals who are (1) in imminent danger of death, (2). Web download the medical records release form.
Web ohio provides compassionate release through judicial release1 and release as if on parole2 to eligible incarcerated individuals who are (1) in imminent danger of death, (2). There are three ways to request information from your medical record regarding your care at ohio state. Developed by lawyers, customized by you. Entry authorizing release of medical records and medical billing records; That treatment from or payment of my claim will not to be impacted by. Web a catalog of ohio department of health program forms. Be prepared to upload a copy of your photo id. Tailored to fit your unique situation. Corrections/erasures void this form please use black or blue ink. Type in your search keywords and hit enter to submit or escape to close
Application to release medical records and medical billing records; While this form was developed by odm, this form can be used in any situation that needs a hipaa or 42 c.f.r. Ad templates built by legal professionals. • please sign and date the form, and send it to the customer service office. Web ohio provides compassionate release through judicial release1 and release as if on parole2 to eligible incarcerated individuals who are (1) in imminent danger of death, (2). Do not alter this form. Probate court of _____ county, ohio _____, judge. Web a catalog of ohio department of health program forms. Web use an online medical record request form to submit your request electronically. Of service to be released:
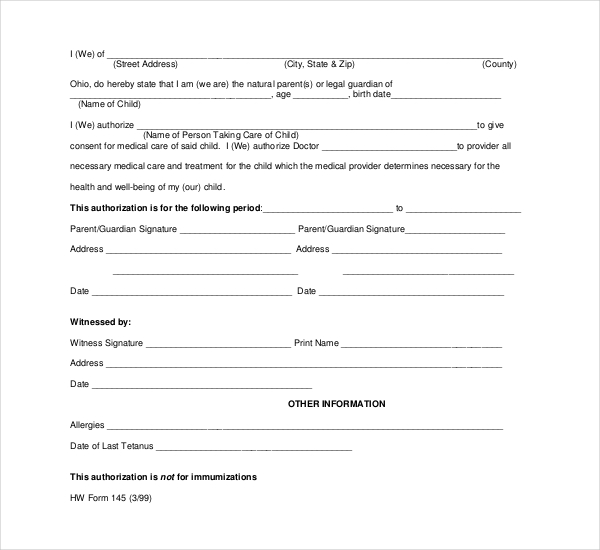
FREE 10+ Sample Child Medical Consent Forms in PDF Excel Word
Tailored to fit your unique situation. Web general consent for medical treatment and permission to release information for billing. Legally binding information release authorization. Developed by lawyers, customized by you. Web use an online medical record request form to submit your request electronically.

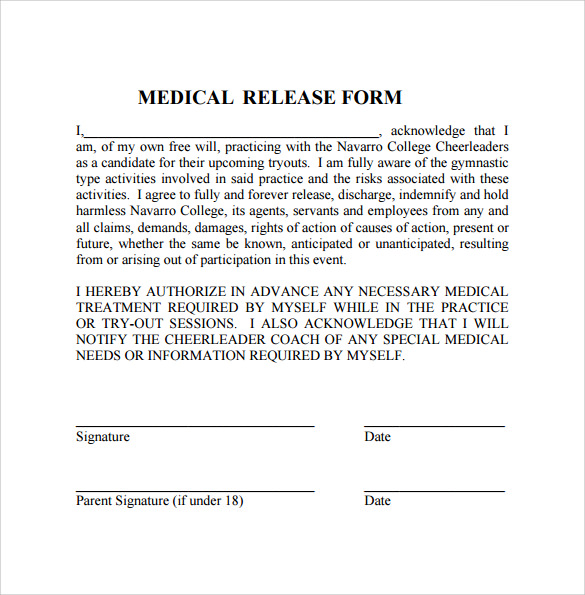
FREE 27+ Sample Medical Release Forms in PDF Excel MS Word
There are three ways to request information from your medical record regarding your care at ohio state. That treatment from or payment of my claim will not to be impacted by. Ad templates built by legal professionals. Try it for free now! To obtain a copy of your medical records from a university hospitals inpatient facility or outpatient facility, please.

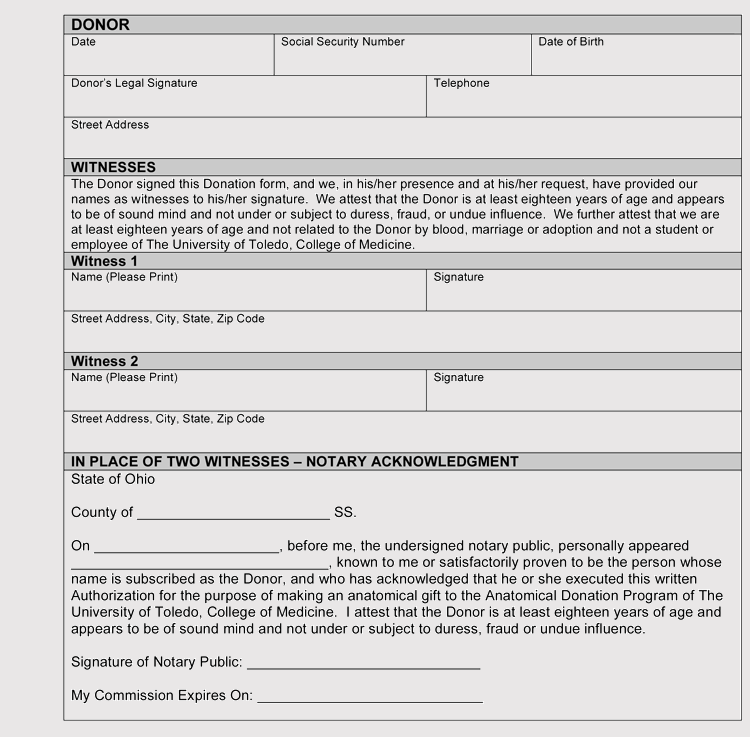
3+ Ohio Do Not Resuscitate Form Free Download
That treatment from or payment of my claim will not to be impacted by. Web type in your search keywords and hit enter to submit or escape to close Web home medical release form — ohio use this form to request your medical records from american health network (ahn) or to ask ahn to send your records to another facility..

Ohio Medical Release Form Download Free Printable Blank Legal Medical
Developed by lawyers, customized by you. Be prepared to upload a copy of your photo id. To obtain a copy of your medical records from a university hospitals inpatient facility or outpatient facility, please contact the. If you are requesting on behalf of the patient,. While this form was developed by odm, this form can be used in any situation.
FREE 10+ Sample Medical Release Forms in PDF MS Word
Web • list the provider(s) you are authorizing to release medical records in the space indicated on this form. Web how to request your medical records. To obtain a copy of your medical records from a university hospitals inpatient facility or outpatient facility, please contact the. Ad register and subscribe now to work on release of medical information & more.
43 FREE Medical Record Release Forms (Consent) Word, PDF
Complete all fields on the authorization form when requesting the release of your records. Web • list the provider(s) you are authorizing to release medical records in the space indicated on this form. That treatment from or payment of my claim will not to be impacted by. There are three ways to request information from your medical record regarding your.
Free Ohio Medical Release Form PDF 63KB 1 Page(s)
Ad templates built by legal professionals. Web download the medical records release form. Type in your search keywords and hit enter to submit or escape to close Of service to be released: Entry authorizing release of medical records and medical billing records;

Hipaa Authorization Form Ohio Captions Trend
Web a catalog of ohio department of health program forms. Web watch newsmax live for the latest news and analysis on today's top stories, right here on facebook. I understand that i have the right to make informed decisions about my health care. Web how to request your medical records. Web • list the provider(s) you are authorizing to release.
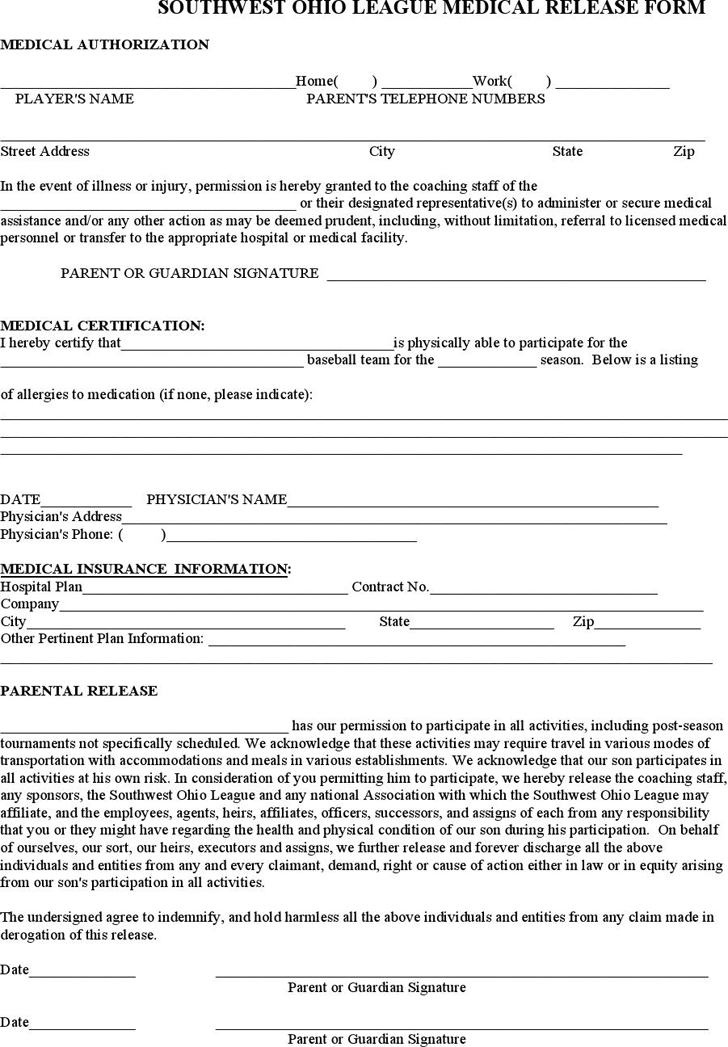
Free Ohio Youth Medical Release Form PDF 25KB 3 Page(s)
Of service to be released: Web use an online medical record request form to submit your request electronically. Web ohio provides compassionate release through judicial release1 and release as if on parole2 to eligible incarcerated individuals who are (1) in imminent danger of death, (2). There are three ways to request information from your medical record regarding your care at.

Free Ohio Medical Records Release Form PDF 166KB 2 Page(s)
Web type in your search keywords and hit enter to submit or escape to close Web home medical release form — ohio use this form to request your medical records from american health network (ahn) or to ask ahn to send your records to another facility. Web use an online medical record request form to submit your request electronically. That.
While This Form Was Developed By Odm, This Form Can Be Used In Any Situation That Needs A Hipaa Or 42 C.f.r.
Complete all fields on the authorization form when requesting the release of your records. Application to release medical records and medical billing records; Legally binding information release authorization. Type in your search keywords and hit enter to submit or escape to close
Web Use The Links Above To Access, Print, And Complete The Authorization Form.
Probate court of _____ county, ohio _____, judge. Web • list the provider(s) you are authorizing to release medical records in the space indicated on this form. Be prepared to upload a copy of your photo id. Web use an online medical record request form to submit your request electronically.
Of Service To Be Released:
Web download the medical records release form. If you are requesting on behalf of the patient,. Ad register and subscribe now to work on release of medical information & more fillable forms. Entry authorizing release of medical records and medical billing records;
Web Type In Your Search Keywords And Hit Enter To Submit Or Escape To Close
Web ohio provides compassionate release through judicial release1 and release as if on parole2 to eligible incarcerated individuals who are (1) in imminent danger of death, (2). Do not alter this form. I understand that i have the right to make informed decisions about my health care. Web general consent for medical treatment and permission to release information for billing.