Patient Authorization Form Generali
Patient Authorization Form Generali - Sign it in a few clicks draw. Please type or print and include all requested information. Instructions for filing a medical claim. Web health insurance medical claim form. Web patient authorization form signature of patient or authorized person date: Use get form or simply click on the template preview to open it in the editor. A patient authorization form is a document authorizing a healthcare provider to share a patient’s medical history with a third party. Web patient authorizationform requiredpatient's last name: Start here to file your travel insurance claim online or contact our claims group. Incomplete forms will be returned unprocessed.
Use get form or simply click on the template preview to open it in the editor. Please type or print and include all requested information. Web patient authorizationform requiredpatient's last name: Incomplete forms will be returned unprocessed. Start here to file your travel insurance claim online or contact our claims group. Incomplete forms will be returned unprocessed. / / ©2020 exelixis, inc. Web up to $40 cash back 01 to fill out the patient authorization form for generali, you will need the following information and documents: All required fields (*) must be completed. Web instructions for completing hrsa authorization for use or disclosure of health information type or print legibly in all fields using dark.
Get patient authorization form generali get form show details on required for all hospital admissions, outpatient surgery, rehab treatment, chemotherapy, radiation. Patient / insured details medical institution details first and last name: All required fields (*) must be completed. This information may be redisclosed if the. Sign it in a few clicks draw. / / ©2020 exelixis, inc. Web patient authorization form signature of patient or authorized person date: Incomplete forms will be returned unprocessed. Web generali is committed to providing prompt, fair and equitable claims service. Web up to $40 cash back 01 to fill out the patient authorization form for generali, you will need the following information and documents:

Free Patient Authorization Forms (Word PDF) WordLayouts
Start here to file your travel insurance claim online or contact our claims group. / / ©2020 exelixis, inc. All required fields (*) must be completed. Get patient authorization form generali get form show details on required for all hospital admissions, outpatient surgery, rehab treatment, chemotherapy, radiation. Please type or print and include all requested information.
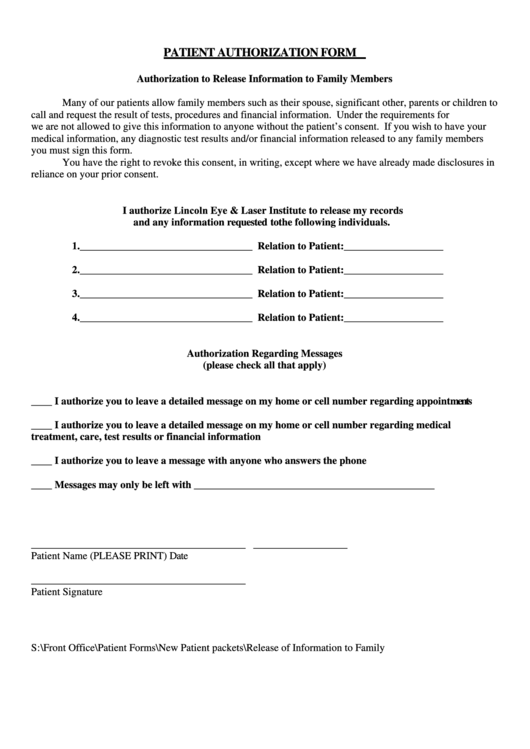
Patient Authorization Form Authorization To Release Information To
All required fields (*) must be completed. Web up to $40 cash back 01 to fill out the patient authorization form for generali, you will need the following information and documents: A patient authorization form is a document authorizing a healthcare provider to share a patient’s medical history with a third party. Incomplete forms will be returned unprocessed. Web health.
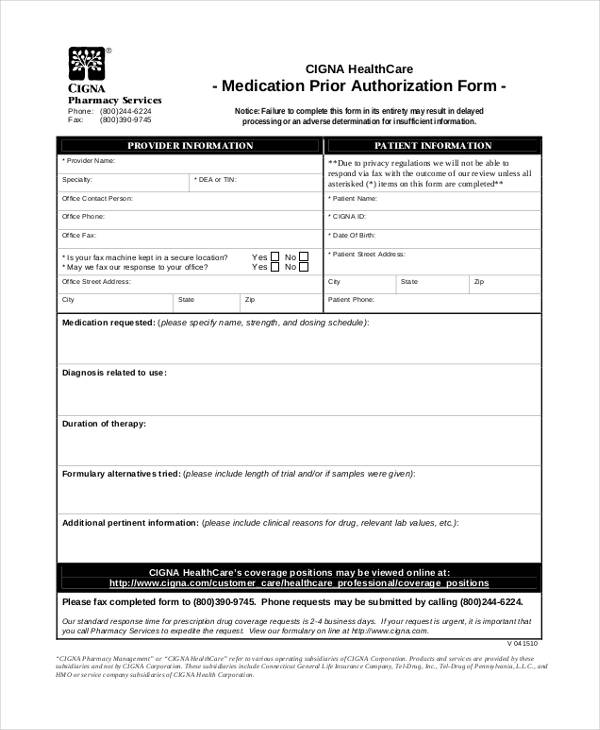
FREE 13+ Prior Authorization Forms in PDF MS Word
Web instructions for completing hrsa authorization for use or disclosure of health information type or print legibly in all fields using dark. Web patient authorization form signature of patient or authorized person date: Web by signing this authorization form, i am authorizing the use or disclosure of my protected health information as described above. Get patient authorization form generali get.
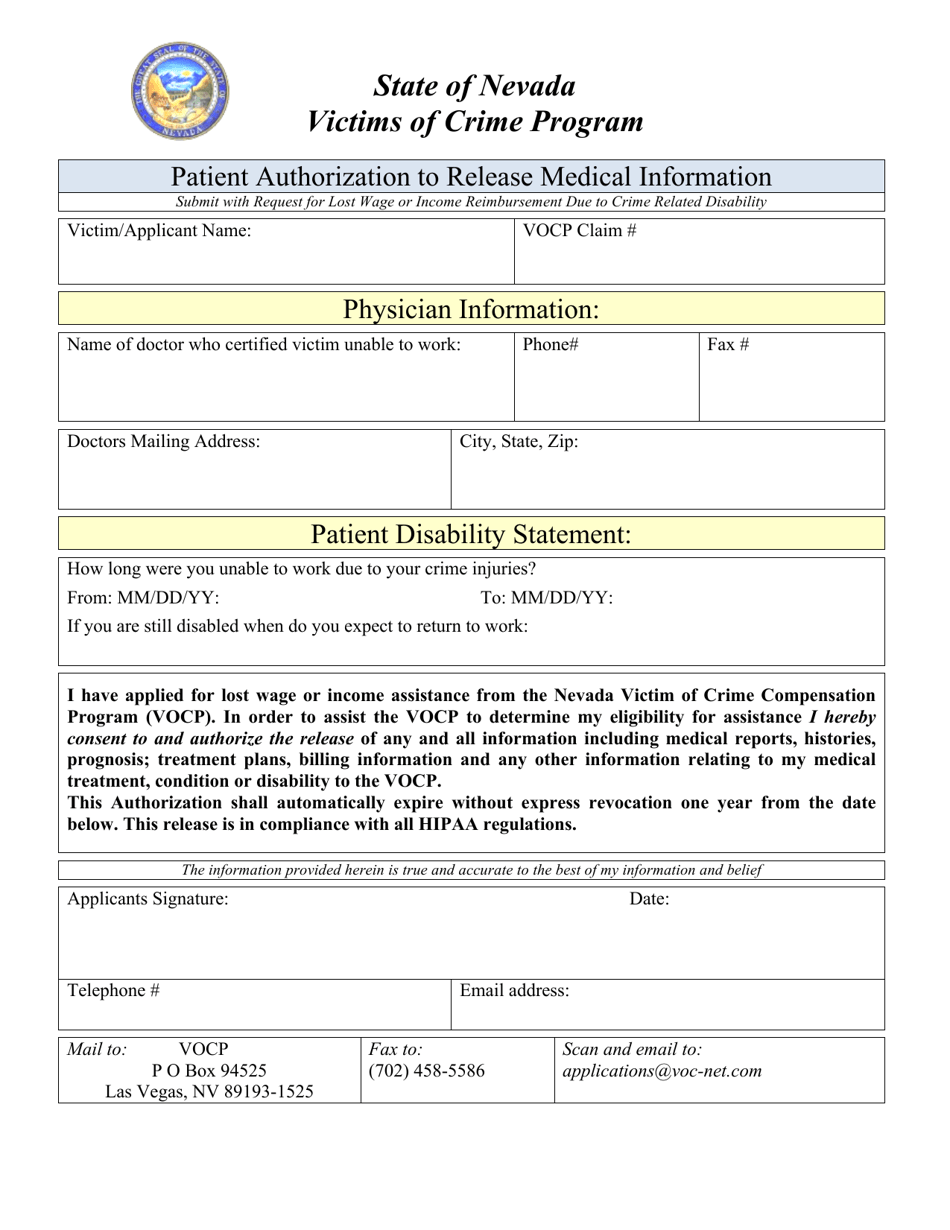
Nevada Patient Authorization to Release Medical Information Download
Web a patient authorization form must be obtained from the patient for phi to be shared for any reasons other than tpo and the other exemptions. Web up to $40 cash back 01 to fill out the patient authorization form for generali, you will need the following information and documents: Please type or print and include all requested information. This.
![[PDF] Future Generali Claim Form For Cashless Facility PDF Download in](https://instapdf.in/wp-content/uploads/pdf-thumbnails/future-generali-claim-form-for-cashless-facility-949.jpg)
[PDF] Future Generali Claim Form For Cashless Facility PDF Download in
Use get form or simply click on the template preview to open it in the editor. Web patient authorization form signature of patient or authorized person date: Edit your patient authorization form generali online type text, add images, blackout confidential details, add comments, highlights and more. This information may be redisclosed if the. Web what is the patient authorization form?
FREE 8+ Sample Medical Authorization Release Forms in MS Word PDF
Please type or print and include all requested information. Web patient authorizationform requiredpatient's last name: Start here to file your travel insurance claim online or contact our claims group. This information may be redisclosed if the. All required fields (*) must be completed.

Printable Patient Authorization Form Template Word
Web patient authorizationform requiredpatient's last name: Web medical treatment authorization form to be filled out by the insured: Instructions for filing a medical claim. The insured employee should fill out part i, either for. Start here to file your travel insurance claim online or contact our claims group.
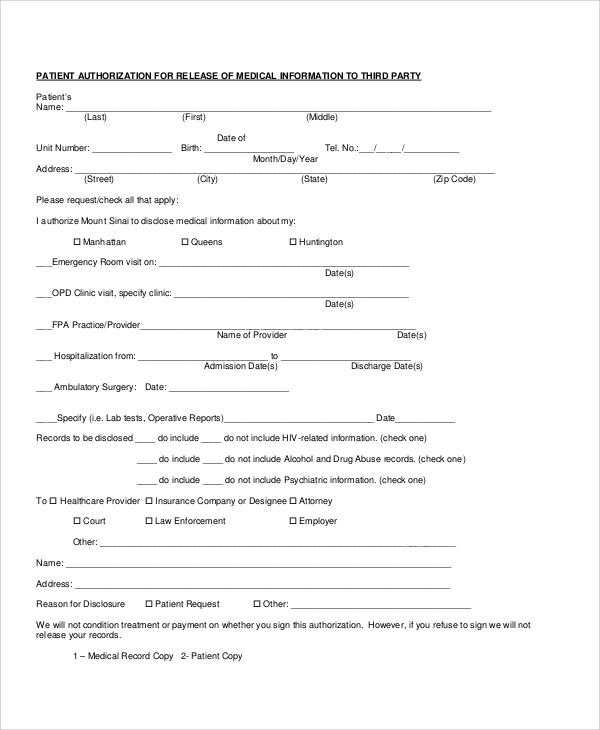
Patient Authorization For The Release Of Medical Information Form
The insured employee should fill out part i, either for. Web instructions for completing hrsa authorization for use or disclosure of health information type or print legibly in all fields using dark. Web by signing this authorization form, i am authorizing the use or disclosure of my protected health information as described above. A patient authorization form is a document.
FREE 22+ Sample Medical Forms in PDF Excel Word
Web health insurance medical claim form. Please type or print and include all requested information. Use get form or simply click on the template preview to open it in the editor. A patient authorization form is a document authorizing a healthcare provider to share a patient’s medical history with a third party. Web by signing this authorization form, i am.
Fillable Patient Authorization To Obtain Outside Medical Records Form
All required fields (*) must be completed. Web medical treatment authorization form to be filled out by the insured: Web by signing this authorization form, i am authorizing the use or disclosure of my protected health information as described above. Web a patient authorization form must be obtained from the patient for phi to be shared for any reasons other.
Web A Patient Authorization Form Must Be Obtained From The Patient For Phi To Be Shared For Any Reasons Other Than Tpo And The Other Exemptions.
Patient / insured details medical institution details first and last name: Web medical treatment authorization form to be filled out by the insured: Edit your patient authorization form generali online type text, add images, blackout confidential details, add comments, highlights and more. Incomplete forms will be returned unprocessed.
Web By Signing This Authorization Form, I Am Authorizing The Use Or Disclosure Of My Protected Health Information As Described Above.
Web patient authorizationform requiredpatient's last name: Instructions for filing a medical claim. Use get form or simply click on the template preview to open it in the editor. Web generali is committed to providing prompt, fair and equitable claims service.
Start Here To File Your Travel Insurance Claim Online Or Contact Our Claims Group.
A patient authorization form is a document authorizing a healthcare provider to share a patient’s medical history with a third party. Web instructions for completing hrsa authorization for use or disclosure of health information type or print legibly in all fields using dark. Get patient authorization form generali get form show details on required for all hospital admissions, outpatient surgery, rehab treatment, chemotherapy, radiation. Web up to $40 cash back 01 to fill out the patient authorization form for generali, you will need the following information and documents:
Relationship/Reason Patient Is Unable To Sign Patient Authorization Form_15693_0414.
Sign it in a few clicks draw. Please type or print and include all requested information. Web patient authorization form signature of patient or authorized person date: All required fields (*) must be completed.