Shiftmed Physical Form
Shiftmed Physical Form - Web who will need access to the shiftmed portal? As an employee of shiftmed, please fill out this form only if you have worked a shift that requires adjustment. | shiftmed is a digital community where the healthcare industry can thrive. Web physical form to be filled out by physician name date of exam height weight b/p pulse vision right 20/ left 20/tb test date done results physician comments:. Web click the apply now button to begin the application process. Registered nurse job description required document checklist clinical evaluation medical forms: Web up to $40 cash back 01. To formally ask or request for time or shift to be changed. Indicate the start and end time of the. Physicians statement tuberculosis screening questionnaire.
Web request forms are used for the following purposes: Registered nurse job description required document checklist clinical evaluation medical forms: Web physical form to be filled out by physician name date of exam height weight b/p pulse vision right 20/ left 20/tb test date done results physician comments:. Complete the online application form, which may include providing your personal information, work. Web no matter what type of nurse you are, anyone who wants to work with shiftmed must upload the following documents to the shiftmed app as part of our. Web program prerequisites include orientation, reading and math assessment or verification of high school diploma or ged, red cross criminal background check. Please enter primary and secondary contacts for day, night, and weekend. Specify your name and position or job title for the shift. Please note, since this is a manual submission,. Web click the apply now button to begin the application process.
Indicate the start and end time of the. Sign it in a few clicks draw your. Work where you want, when you want! Web shiftmed | 62,147 followers on linkedin. Type text, complete fillable fields, insert images, highlight. Web request forms are used for the following purposes: Edit your shift change form template form online. Web program prerequisites include orientation, reading and math assessment or verification of high school diploma or ged, red cross criminal background check. Please do not write in “examining facility use only” areas. Web edit your printable physical exam form online type text, add images, blackout confidential details, add comments, highlights and more.

Free Physical Form for Work How to Fill Out (with Examples) Word PDF
Web program prerequisites include orientation, reading and math assessment or verification of high school diploma or ged, red cross criminal background check. Web physical form to be filled out by physician name date of exam height weight b/p pulse vision right 20/ left 20/tb test date done results physician comments:. Complete the online application form, which may include providing your.
Physical Form Printable Printable Forms Free Online
Web find out what works well at shiftmed from the people who know best. Specify your name and position or job title for the shift. To request for a person to be the reliever or the replacement for the. Web program prerequisites include orientation, reading and math assessment or verification of high school diploma or ged, red cross criminal background.

ShiftMed Nursing Jobs by
Web physical form to be filled out by physician name date of exam height weight b/p pulse vision right 20/ left 20/tb test date done results physician comments:. Compare pay for popular roles. Please enter primary and secondary contacts for day, night, and weekend. Edit your shift change form template form online. Web click the apply now button to begin.

Employment Physical form Template New Five Facts that Nobody Medical
As an employee of shiftmed, please fill out this form only if you have worked a shift that requires adjustment. Complete the online application form, which may include providing your personal information, work. Web physical form to be filled out by physician name date of exam height weight b/p pulse vision right 20/ left 20/tb test date done results physician.
FREE 5+ Sample Employee Physical Forms in PDF
Web program prerequisites include orientation, reading and math assessment or verification of high school diploma or ged, red cross criminal background check. Complete the online application form, which may include providing your personal information, work. Web up to $40 cash back get, create, make and sign shift swap form template. Web download the shiftmed app today! First name last name.

Free Physical Form for Work How to Fill Out (with Examples) Word PDF
Sign it in a few clicks draw your. Physicians statement tuberculosis screening questionnaire. Web physical form to be filled out by physician name date of exam height weight b/p pulse vision right 20/ left 20/tb test date done results physician comments:. Indicate the start and end time of the. Compare pay for popular roles.
History And Physical Exam Template Pdf PDF Template
Web shiftmed | 62,147 followers on linkedin. Web no matter what type of nurse you are, anyone who wants to work with shiftmed must upload the following documents to the shiftmed app as part of our. | shiftmed is a digital community where the healthcare industry can thrive. Please note, since this is a manual submission,. Web program prerequisites include.

Pre Employment Physical form Template Unique Best Dynamite Printable
(select add new contact for additional users) *. Web find out what works well at shiftmed from the people who know best. Web up to $40 cash back get, create, make and sign shift swap form template. Please note, since this is a manual submission,. March 2019 medical examination and history report selectees:

Employee Physical Exam form Template Elegant Pre Employment Physical
Start by entering the date and time of the shift. First name last name email phone number certificate or license select. Web find out what works well at shiftmed from the people who know best. Compare pay for popular roles. Web up to $40 cash back 01.
ShiftMed to Hire 5,000 CNAs in Cities Hit Hard by COVID19 Business Wire
Web edit your printable physical exam form online type text, add images, blackout confidential details, add comments, highlights and more. Registered nurse job description required document checklist clinical evaluation medical forms: Type text, complete fillable fields, insert images, highlight. Complete the online application form, which may include providing your personal information, work. Web up to $40 cash back 01.
Indicate The Start And End Time Of The.
To formally ask or request for time or shift to be changed. First name last name email phone number certificate or license select. Web request forms are used for the following purposes: As an employee of shiftmed, please fill out this form only if you have worked a shift that requires adjustment.
Complete The Online Application Form, Which May Include Providing Your Personal Information, Work.
Web find out what works well at shiftmed from the people who know best. Web edit your printable physical exam form online type text, add images, blackout confidential details, add comments, highlights and more. Web shiftmed | 62,147 followers on linkedin. Registered nurse job description required document checklist clinical evaluation medical forms:
Compare Pay For Popular Roles.
Work where you want, when you want! Web no matter what type of nurse you are, anyone who wants to work with shiftmed must upload the following documents to the shiftmed app as part of our. (select add new contact for additional users) *. Web up to $40 cash back 01.
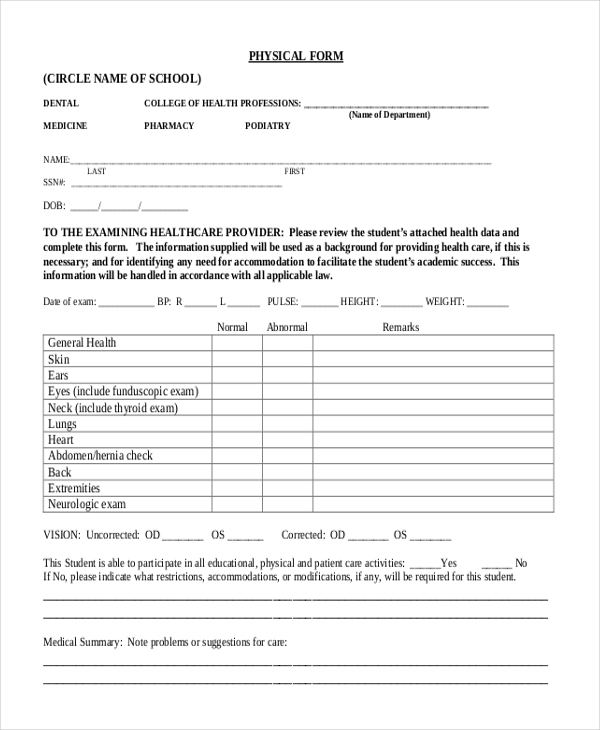
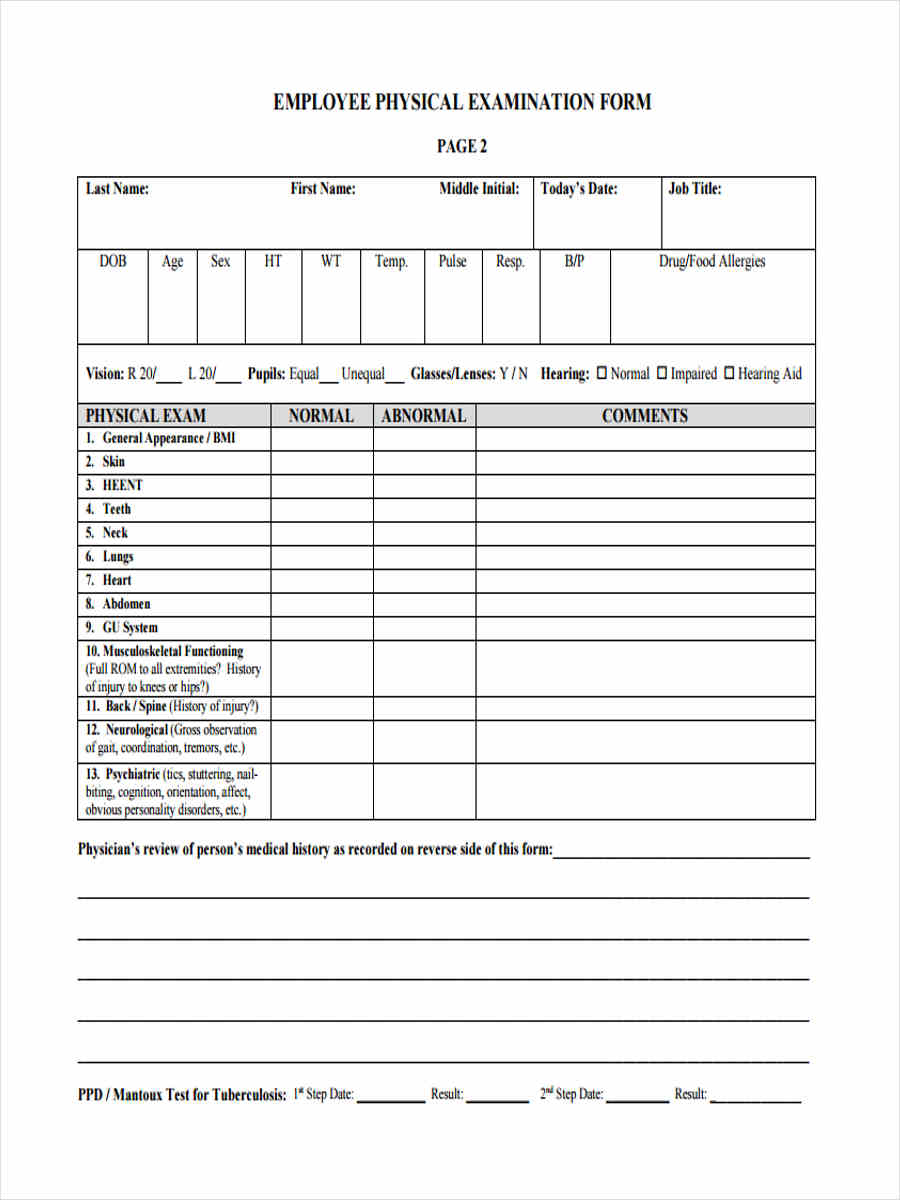
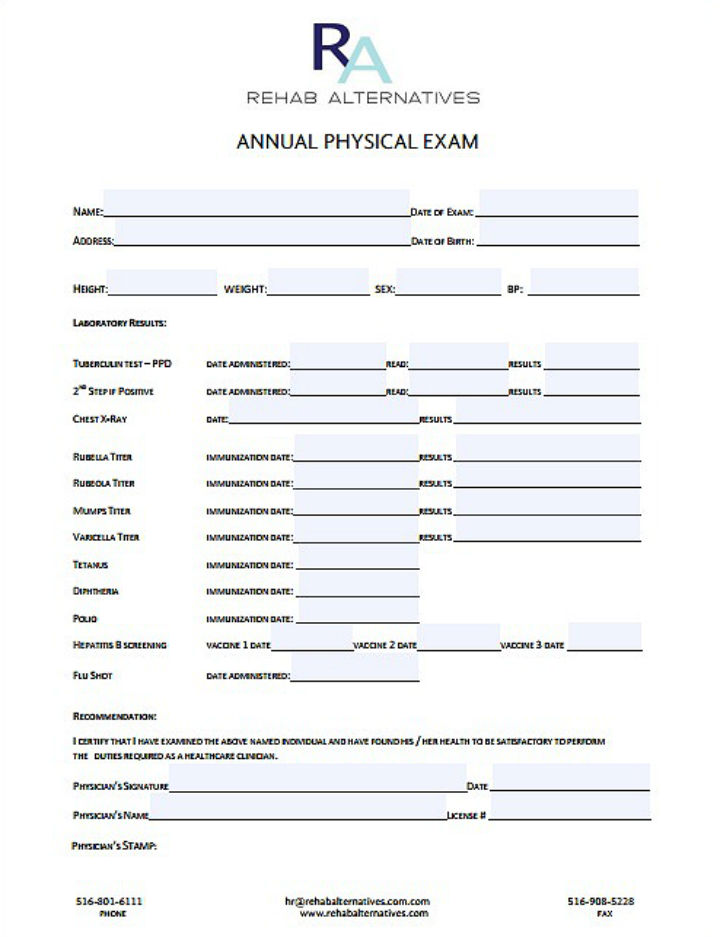
Web Physical Form To Be Filled Out By Physician Name Date Of Exam Height Weight B/P Pulse Vision Right 20/ Left 20/Tb Test Date Done Results Physician Comments:.
Physicians statement tuberculosis screening questionnaire. Get the inside scoop on jobs, salaries, top office locations, and ceo insights. To request for a person to be the reliever or the replacement for the. Sign it in a few clicks draw your.