Umr Appeal Form
Umr Appeal Form - Medical necessity or infertility this application for first level appeal should be used to appeal adverse benefit determinations involving medical necessity of a particular treatment, procedure, or service/supply, or for any. Web provider how can we help you? You must complete this form and provide all requested information. Please fill out the below information when you are requesting a review of an adverse benefit determination or claim denial by umr. Umr.com > provider > claim appeals. Box 30783 salt lake city, ut. Quickly and easily complete claims, appeal requests and referrals, all from your computer. For help call umr at the number listed on the back of your health plan id card. Web umr application for first level appeal: Please fill out the below information when you are requesting a review of an adverse benefit determination or claim denial by umr.
This letter is generated to alert a provider of an overpayment. Please fill out the below information when you are requesting a review of an adverse benefit determination or claim denial by umr. Web this application for second level appeal should be used to appeal adverse benefit determinations involving medical necessity of a particular treatment, procedure, or service/supply, or for any determination regarding treatment for infertility important notice: Umr.com > provider > claim appeals. Quickly and easily complete claims, appeal requests and referrals, all from your computer. Follow prompts for submitting the inquiry. Web any member or someone who that member names to act as an authorized representative may file an appeal. You must complete this form and provide all requested information. Web some clinical requests for predetermination or prior authorization (i.e., spinal surgery or genetic testing) require specific forms that you must submit with the request. Please fill out the below information when you are requesting a review of an adverse benefit determination or claim denial by umr.
If you are appealing on behalf of someone else, please also include the designation of authorized representative form with this request. Web this application for second level appeal should be used to appeal adverse benefit determinations involving medical necessity of a particular treatment, procedure, or service/supply, or for any determination regarding treatment for infertility important notice: Quickly and easily complete claims, appeal requests and referrals, all from your computer. If you are appealing on behalf of someone else, please also include the designation of authorized representative form with this request. You must complete this form and provide all requested information. Box 30783 salt lake city, ut. Umr.com > provider > claim appeals. Web umr application for first level appeal: Yes, you may give us additional information supporting your claim. Find clinical request forms at umr.com > provider > find a form open_in_new.

Umr Appeal Form Fill Online, Printable, Fillable, Blank pdfFiller
If you are appealing on behalf of someone else, please also include the designation of authorized representative form with this request. Web this application for second level appeal should be used to appeal adverse benefit determinations involving medical necessity of a particular treatment, procedure, or service/supply, or for any determination regarding treatment for infertility important notice: Web any member or.
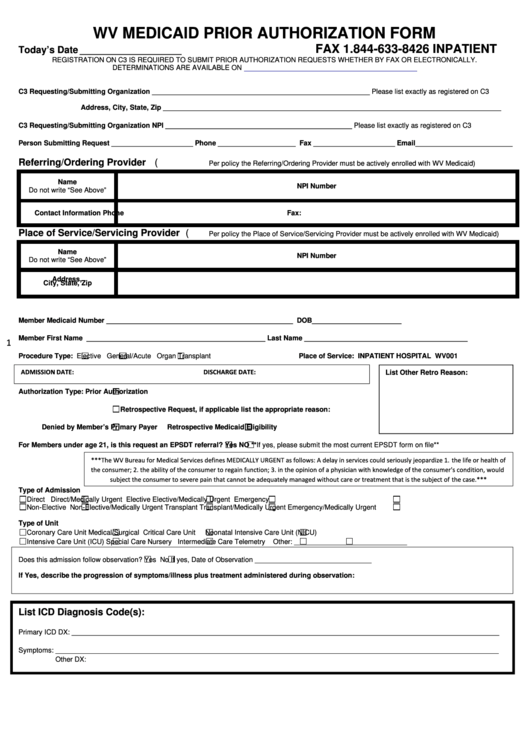
Wv Medicaid Prior Authorization Form (Inpatient) printable pdf download
Web umr application for first level appeal: Yes, you may give us additional information supporting your claim. You must complete this form and provide all requested information. In addition, a corresponding remittance notification is created for additional notification. Call the number listed on the back of the member id card.

UMR EZ Claim Form Medical/Vision Fill and Sign Printable Template
Web any member or someone who that member names to act as an authorized representative may file an appeal. Medical necessity or infertility this application for first level appeal should be used to appeal adverse benefit determinations involving medical necessity of a particular treatment, procedure, or service/supply, or for any. Please fill out the below information when you are requesting.
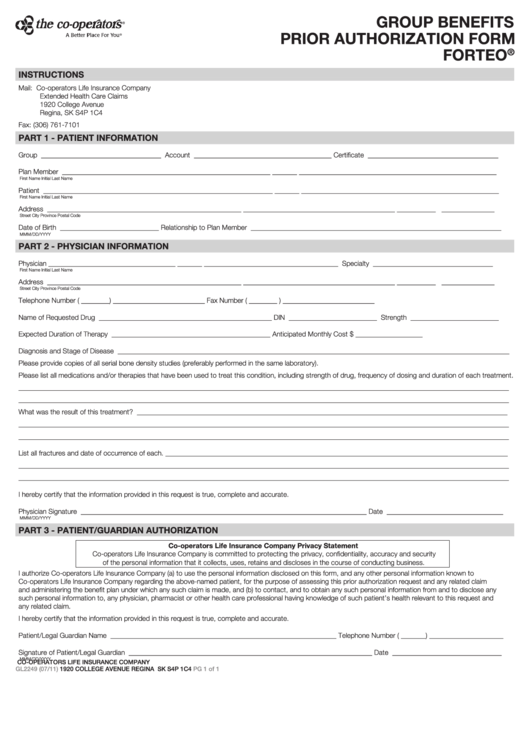
Fillable Form Gl2249 Group Benefits Prior Authorization Xolair
Web provider how can we help you? Web attach all supporting materials to the request, including member specific treatment plans or clinical records (the decision is based on the materials you provide) umr. Find clinical request forms at umr.com > provider > find a form open_in_new. Can i provide additional information about my claim? Web umr application for first level.
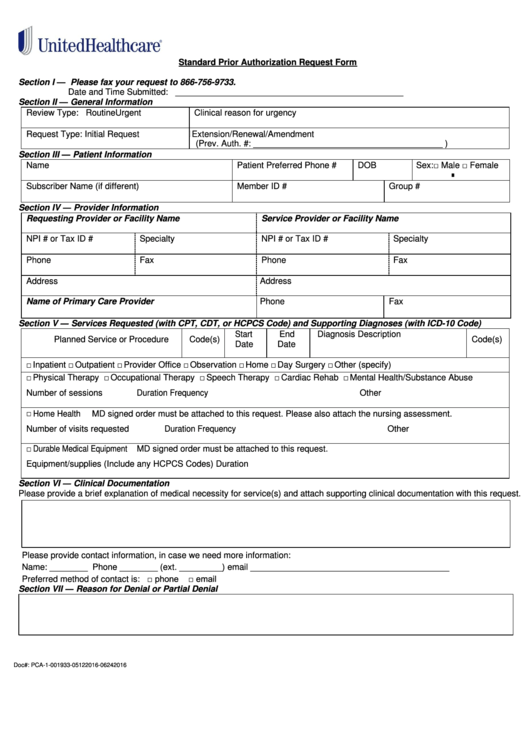
Fillable Standard Prior Authorization Request Form United Healthcare
If you are appealing on behalf of someone else, please also include the designation of authorized representative form with this request. Web umr application for first level appeal: Web attach all supporting materials to the request, including member specific treatment plans or clinical records (the decision is based on the materials you provide) umr. Web provider how can we help.
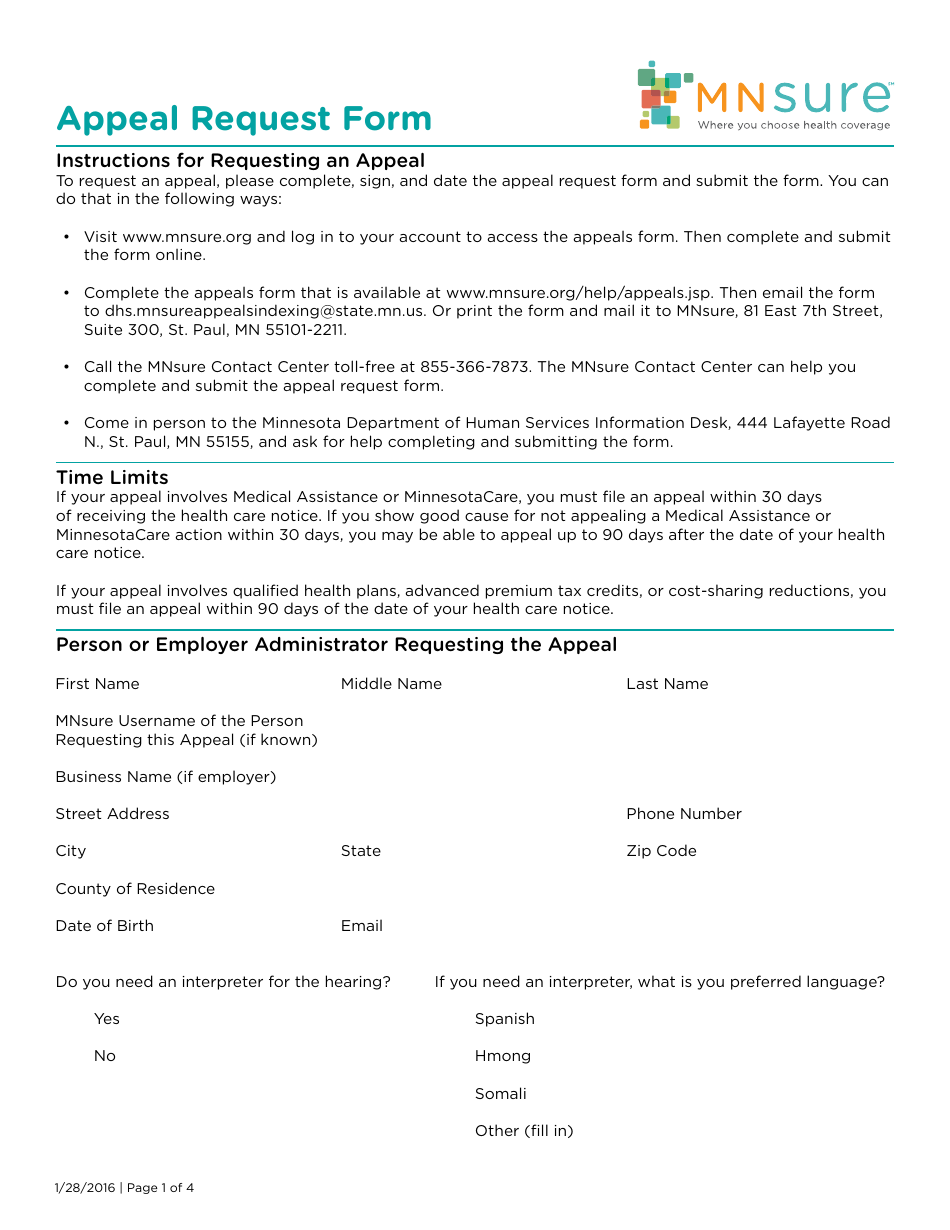
Minnesota Appeal Request Form Mnsure Download Fillable PDF
Can i provide additional information about my claim? In addition, a corresponding remittance notification is created for additional notification. Web you have access to the most common umr forms right at your fingertips. If you are appealing on behalf of someone else, please also include the designation of authorized representative form with this request. Web provider how can we help.
Fillable Notice Of Appeal To The Alabama Court Of Criminal Appeals Form
In addition, a corresponding remittance notification is created for additional notification. Web provider how can we help you? Web any member or someone who that member names to act as an authorized representative may file an appeal. Find clinical request forms at umr.com > provider > find a form open_in_new. Web some clinical requests for predetermination or prior authorization (i.e.,.

University Of Maryland Global Campus Dependent Student Special
Web this application for second level appeal should be used to appeal adverse benefit determinations involving medical necessity of a particular treatment, procedure, or service/supply, or for any determination regarding treatment for infertility important notice: Call the number listed on the back of the member id card. Follow prompts for submitting the inquiry. If you are appealing on behalf of.
Free UnitedHealthcare Prior (Rx) Authorization Form PDF eForms
For help call umr at the number listed on the back of your health plan id card. Web provider how can we help you? This letter is generated to alert a provider of an overpayment. In addition, a corresponding remittance notification is created for additional notification. Can i provide additional information about my claim?
Sample Caremark Prior Authorization Form 8+ Free Documents in PDF
Please fill out the below information when you are requesting a review of an adverse benefit determination or claim denial by umr. Follow prompts for submitting the inquiry. Umr.com > provider > claim appeals. Web this application for second level appeal should be used to appeal adverse benefit determinations involving medical necessity of a particular treatment, procedure, or service/supply, or.
Medical Necessity Or Infertility This Application For First Level Appeal Should Be Used To Appeal Adverse Benefit Determinations Involving Medical Necessity Of A Particular Treatment, Procedure, Or Service/Supply, Or For Any.
Call the number listed on the back of the member id card. Please fill out the below information when you are requesting a review of an adverse benefit determination or claim denial by umr. Web you have access to the most common umr forms right at your fingertips. Web attach all supporting materials to the request, including member specific treatment plans or clinical records (the decision is based on the materials you provide) umr.
Web Some Clinical Requests For Predetermination Or Prior Authorization (I.e., Spinal Surgery Or Genetic Testing) Require Specific Forms That You Must Submit With The Request.
Can i provide additional information about my claim? Quickly and easily complete claims, appeal requests and referrals, all from your computer. Web umr application for first level appeal: Box 30783 salt lake city, ut.
Web Any Member Or Someone Who That Member Names To Act As An Authorized Representative May File An Appeal.
Web this application for second level appeal should be used to appeal adverse benefit determinations involving medical necessity of a particular treatment, procedure, or service/supply, or for any determination regarding treatment for infertility important notice: This letter is generated to alert a provider of an overpayment. You must complete this form and provide all requested information. Web provider how can we help you?
For Help Call Umr At The Number Listed On The Back Of Your Health Plan Id Card.
If you are appealing on behalf of someone else, please also include the designation of authorized representative form with this request. If you are appealing on behalf of someone else, please also include the designation of authorized representative form with this request. Find clinical request forms at umr.com > provider > find a form open_in_new. Follow prompts for submitting the inquiry.