Umr Provider Appeal Form
Umr Provider Appeal Form - Sign it in a few clicks. The following links provide information including, but not limited to, prior authorization, processing claims, protocol, contact. Type text, add images, blackout confidential details, add comments, highlights and more. Web appeal should be sent to: This letter is generated to alert a provider of an overpayment. There is no cost to you for these copies. Your appeal must include the following: Web quickly and easily complete claims, appeal requests and referrals, all from your computer. Please fill out the below information when you are requesting a review of an adverse benefit determination or claim denial by umr. Please fill out the below information when you are requesting a review of an adverse benefit determination or claim denial by umr.
Sign it in a few clicks. Send your request to the address provided in the initial denial letter or eob. Web quickly and easily complete claims, appeal requests and referrals, all from your computer. Edit your umr post service appeal form online. Please fill out the below information when you are requesting a review of an adverse benefit determination or claim denial by umr. This letter is generated to alert a provider of an overpayment. What happens if i don’t agree with the outcome of my. Web select the orange get form button to begin editing and enhancing. Attach all supporting materials to the request, including member specific treatment plans or clinical records (the decision is based on the. Web some clinical requests for predetermination or prior authorization (i.e., spinal surgery or genetic testing) require specific forms that you must submit with the request.
Sign it in a few clicks. Please fill out the below information when you are requesting a review of an adverse benefit determination or claim denial by umr. Web appeal should be sent to: You must file this first level appeal within 180 days of the date you receive notice of the adverse benefit determination from the network/claim. Send your request to the address provided in the initial denial letter or eob. The following links provide information including, but not limited to, prior authorization, processing claims, protocol, contact. Web provider name, address and tin; Web quickly and easily complete claims, appeal requests and referrals, all from your computer. There is no cost to you for these copies. This letter is generated to alert a provider of an overpayment.
Umr Prior Authorization Form Fill Out and Sign Printable PDF Template
You must file this first level appeal within 180 days of the date you receive notice of the adverse benefit determination from the network/claim. Turn on the wizard mode on the top toolbar to acquire extra recommendations. Web select the orange get form button to begin editing and enhancing. • complete, date, and sign this application for first level appeal.
Nj Dobicappcar Form Fill Out and Sign Printable PDF Template signNow
Web levels of appeal are waived. This letter is generated to alert a provider of an overpayment. You must file this first level appeal within 180 days of the date you receive notice of the adverse benefit determination from the network/claim. Type text, add images, blackout confidential details, add comments, highlights and more. Medical claim form (hcfa1500) notification form.

Healthsmart Rx Prior Authorization Form Fill and Sign Printable
Please fill out the below information when you are requesting a review of an adverse benefit determination or claim denial by umr. Medical claim form (hcfa1500) notification form. There is no cost to you for these copies. Web appeal should be sent to: The following links provide information including, but not limited to, prior authorization, processing claims, protocol, contact.

Umr Appeal Form Fill Online, Printable, Fillable, Blank pdfFiller
Edit your umr post service appeal form online. Web select the orange get form button to begin editing and enhancing. Easily fill out pdf blank, edit, and sign them. • complete, date, and sign this application for first level appeal (both employee and patient, other. Web some clinical requests for predetermination or prior authorization (i.e., spinal surgery or genetic testing).
Prior Authorization Request Form printable pdf download
Web some clinical requests for predetermination or prior authorization (i.e., spinal surgery or genetic testing) require specific forms that you must submit with the request. Web levels of appeal are waived. This letter is generated to alert a provider of an overpayment. Edit your umr post service appeal form online. Web quickly and easily complete claims, appeal requests and referrals,.
Umr Wellness Guidelines Umr 55 2 Edit Fill Print Download Online
Web levels of appeal are waived. Type text, add images, blackout confidential details, add comments, highlights and more. Edit your umr post service appeal form online. You must file this first level appeal within 180 days of the date you receive notice of the adverse benefit determination from the network/claim. Sign it in a few clicks.
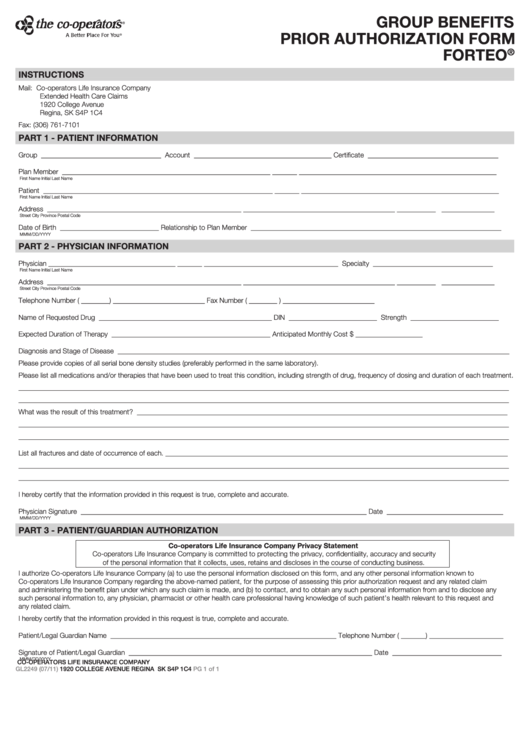
Fillable Form Gl2249 Group Benefits Prior Authorization Xolair
Such recipient shall be liable for using and protecting umr’s proprietary business. Web quickly and easily complete claims, appeal requests and referrals, all from your computer. Web select the orange get form button to begin editing and enhancing. There is no cost to you for these copies. Please fill out the below information when you are requesting a review of.

Forms + Brochures Compass Rose Benefits Group Compass Rose Health Plan
Easily fill out pdf blank, edit, and sign them. Web select the orange get form button to begin editing and enhancing. Turn on the wizard mode on the top toolbar to acquire extra recommendations. Your appeal must include the following: Edit your umr post service appeal form online.
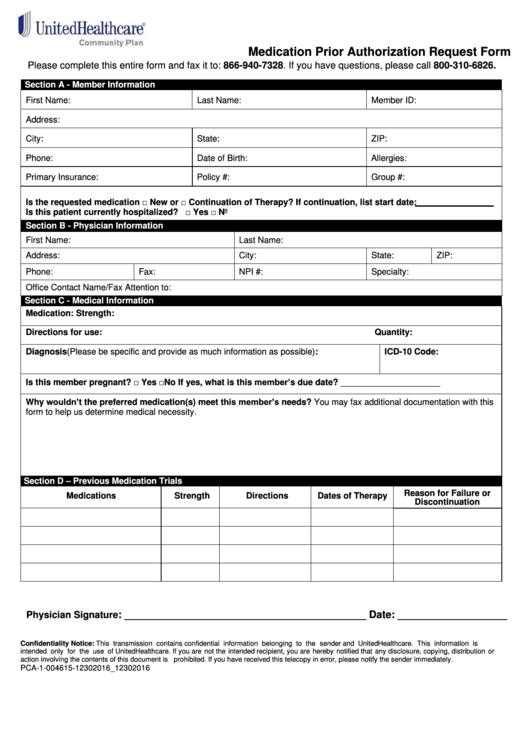
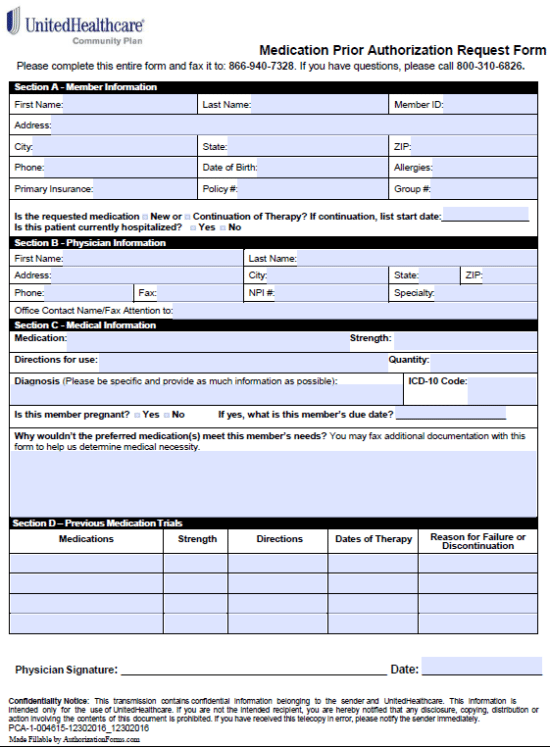
Medication Prior Authorization Request Form United Healthcare
Easily fill out pdf blank, edit, and sign them. Web select the orange get form button to begin editing and enhancing. Web care provider administrative guides and manuals. Please fill out the below information when you are requesting a review of an adverse benefit determination or claim denial by umr. Medical claim form (hcfa1500) notification form.
Free United Healthcare Prior Prescription (Rx) Authorization Form PDF
Call the number listed on. Web quickly and easily complete claims, appeal requests and referrals, all from your computer. Web care provider administrative guides and manuals. Save or instantly send your ready documents. What happens if i don’t agree with the outcome of my.
Medical Claim Form (Hcfa1500) Notification Form.
Such recipient shall be liable for using and protecting umr’s proprietary business. Call the number listed on. Send your request to the address provided in the initial denial letter or eob. Sign it in a few clicks.
Edit Your Umr Post Service Appeal Form Online.
Attach all supporting materials to the request, including member specific treatment plans or clinical records (the decision is based on the. Save or instantly send your ready documents. Easily fill out pdf blank, edit, and sign them. Please fill out the below information when you are requesting a review of an adverse benefit determination or claim denial by umr.
The Following Links Provide Information Including, But Not Limited To, Prior Authorization, Processing Claims, Protocol, Contact.
Web quickly and easily complete claims, appeal requests and referrals, all from your computer. Please fill out the below information when you are requesting a review of an adverse benefit determination or claim denial by umr. Web provider name, address and tin; Your appeal must include the following:
Web Select The Orange Get Form Button To Begin Editing And Enhancing.
Web appeal should be sent to: You must file this first level appeal within 180 days of the date you receive notice of the adverse benefit determination from the network/claim. • complete, date, and sign this application for first level appeal (both employee and patient, other. There is no cost to you for these copies.