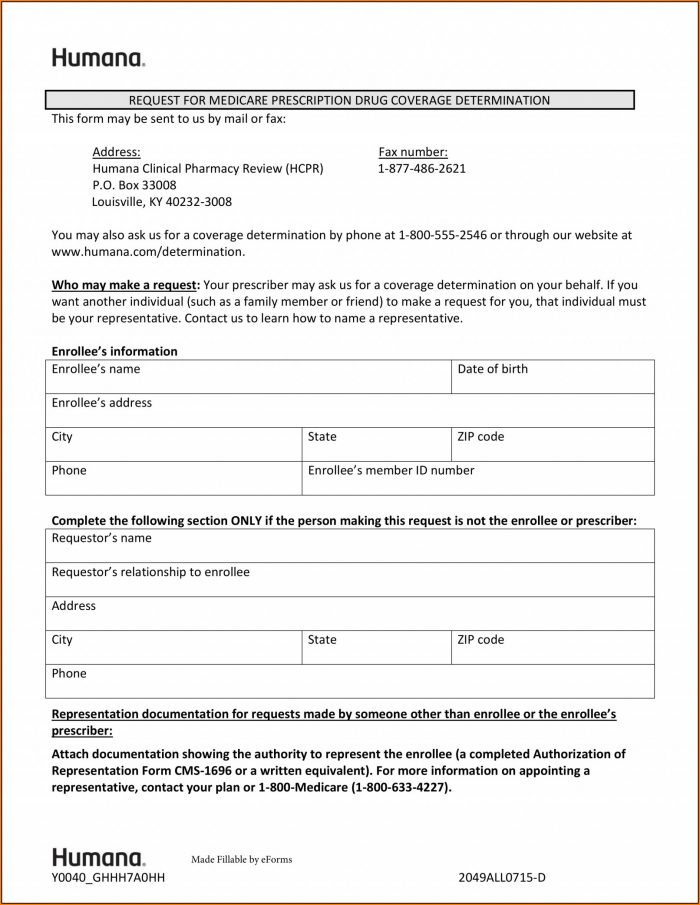
Buckeye Prior Authorization Form Pdf
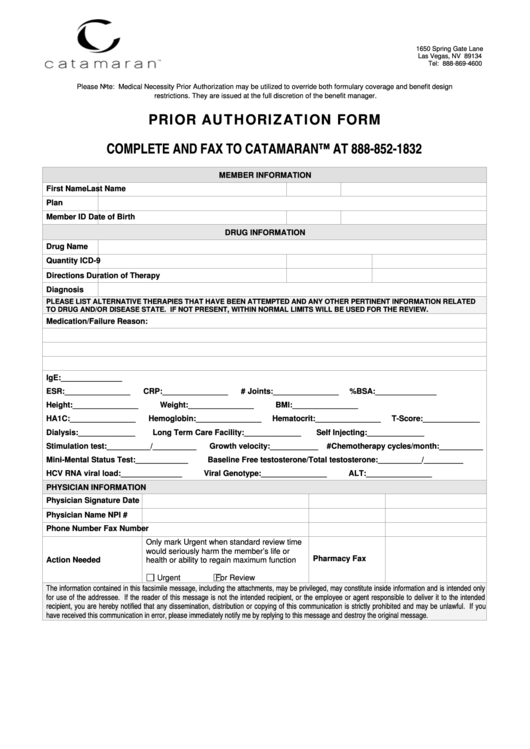
Buckeye Prior Authorization Form Pdf - I certify this request is urgent and medically necessary to. Save time and complete online. Web medication prior authorization request form buckeye community health plan, ohio (do not use this form for biopharmaceutical products) fax this completed. We call this prior authorization. Edit your buckeye mycare prior authorization form online type text, add images, blackout confidential details, add comments, highlights and more. Save or instantly send your ready documents. Use our preferred drug list to find more information on. Easily fill out pdf blank, edit, and sign them. We call this prior authorization(pa). Determination within 10 calendar days of receiving all necessary information.
Prior authorization does not guarantee. Sign it in a few. We call this prior authorization. We require you to get approval from us before we agree to cover certain drugs. Web requesting physician to receive priority. Save or instantly send your ready documents. We call this prior authorization(pa). Web ambetter prior authorization request form. Providers need to send prior authorizations through. If you don’t get approval, you.
We call this prior authorization. If you don’t get approval, you. We call this prior authorization(pa). Edit your buckeye mycare prior authorization form online type text, add images, blackout confidential details, add comments, highlights and more. Web medication prior authorization request form buckeye community health plan, ohio (do not use this form for biopharmaceutical products) fax this completed. Use our preferred drug list to find more information on. Save time and complete online. Indicates required field member information member id * date of birth last name, first(mmddyyyy). Providers need to send prior authorizations through. Web requesting physician to receive priority.
Prior Authorization Form printable pdf download
Sign it in a few. If your drug needs prior authorization, call buckeye health plan. Web medication prior authorization request form buckeye community health plan, ohio (do not use this form for biopharmaceutical products) fax this completed. Save or instantly send your ready documents. Edit your buckeye mycare prior authorization form online type text, add images, blackout confidential details, add.
Free Prior (Rx) Authorization Forms PDF eForms
Please click view all or search by generic or brand name to find the correct prior authorization fax form for. The process of getting prior approval from buckeye as to the appropriateness of a service or medication. Providers need to send prior authorizations through. We call this prior authorization. Edit your buckeye mycare prior authorization form online type text, add.
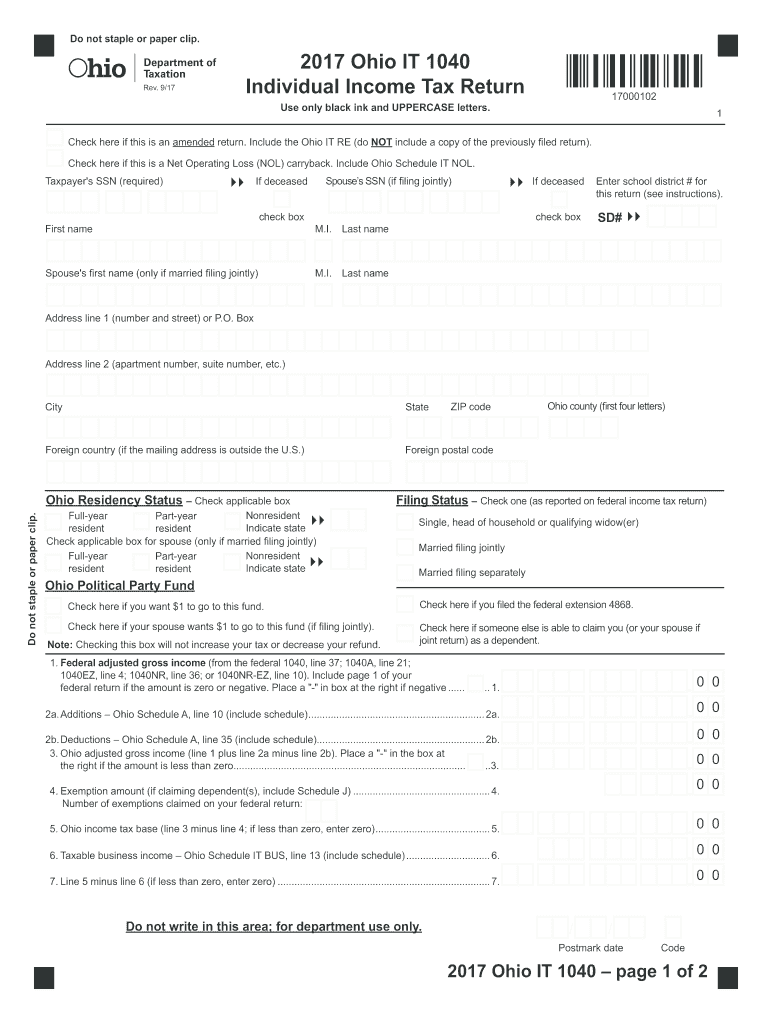
Ohio Tax Forms Fill Out and Sign Printable PDF Template signNow
We require you to get approval from us before we agree to cover certain drugs. If you don’t get approval, you. Web ambetter prior authorization request form. Web requesting physician to receive priority. If your drug needs prior authorization, call buckeye health plan.
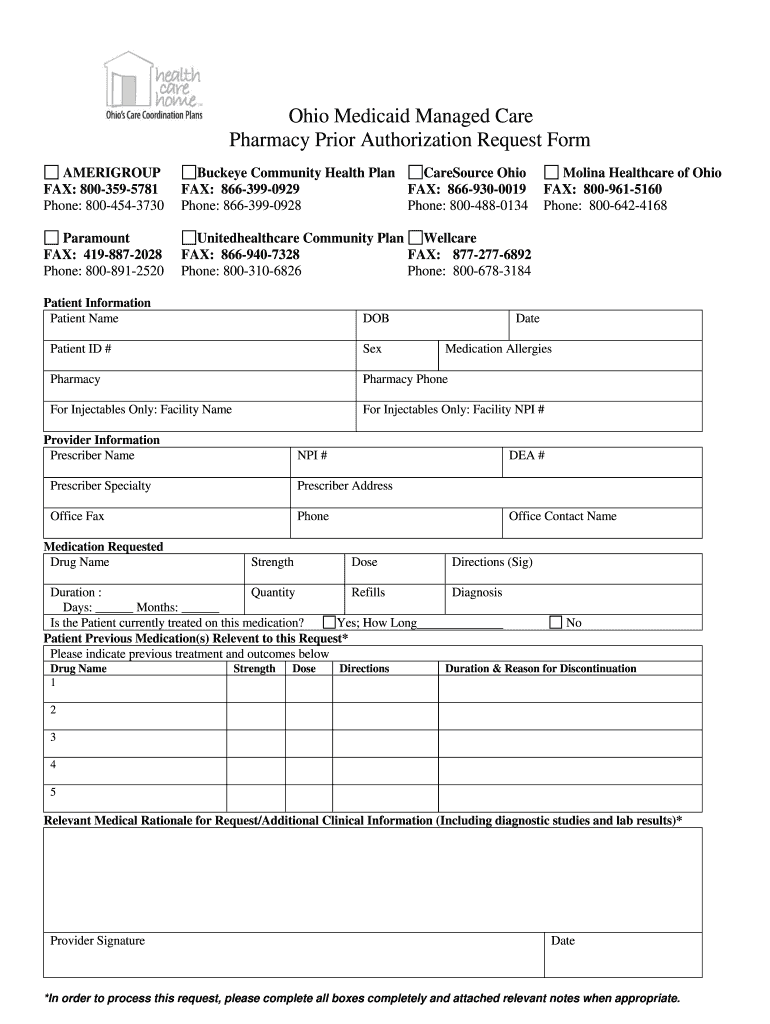
Ohio Medicaid Prior Authorization Form Fill Online, Printable
Providers need to send prior authorizations through. Please click view all or search by generic or brand name to find the correct prior authorization fax form for. If your drug needs prior authorization, call buckeye health plan. Prior authorization does not guarantee. Web complete buckeye mycare prior authorization form online with us legal forms.
Covermymeds Prior Authorization Form Pdf Form Resume Examples
We call this prior authorization. Easily fill out pdf blank, edit, and sign them. Indicates required field member information member id * date of birth last name, first(mmddyyyy). Web medication prior authorization request form buckeye community health plan, ohio (do not use this form for biopharmaceutical products) fax this completed. Edit your buckeye mycare prior authorization form online type text,.
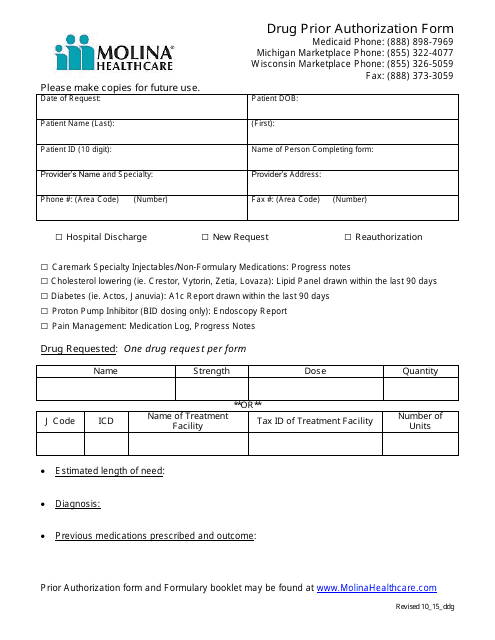
Drug Prior Authorization Form Molina Healthcare Download Printable
Web you must get our okay for certain drugs before using them. Web medication prior authorization request form buckeye community health plan, ohio (do not use this form for biopharmaceutical products) fax this completed. Prior authorization does not guarantee. We require you to get approval from us before we agree to cover certain drugs. Easily fill out pdf blank, edit,.

Bcbs Prior Authorization Form Form Resume Examples NRE34PV36x
Providers need to send prior authorizations through. Save or instantly send your ready documents. Web medication prior authorization request form buckeye community health plan, ohio (do not use this form for biopharmaceutical products) fax this completed. Sign it in a few. Please click view all or search by generic or brand name to find the correct prior authorization fax form.
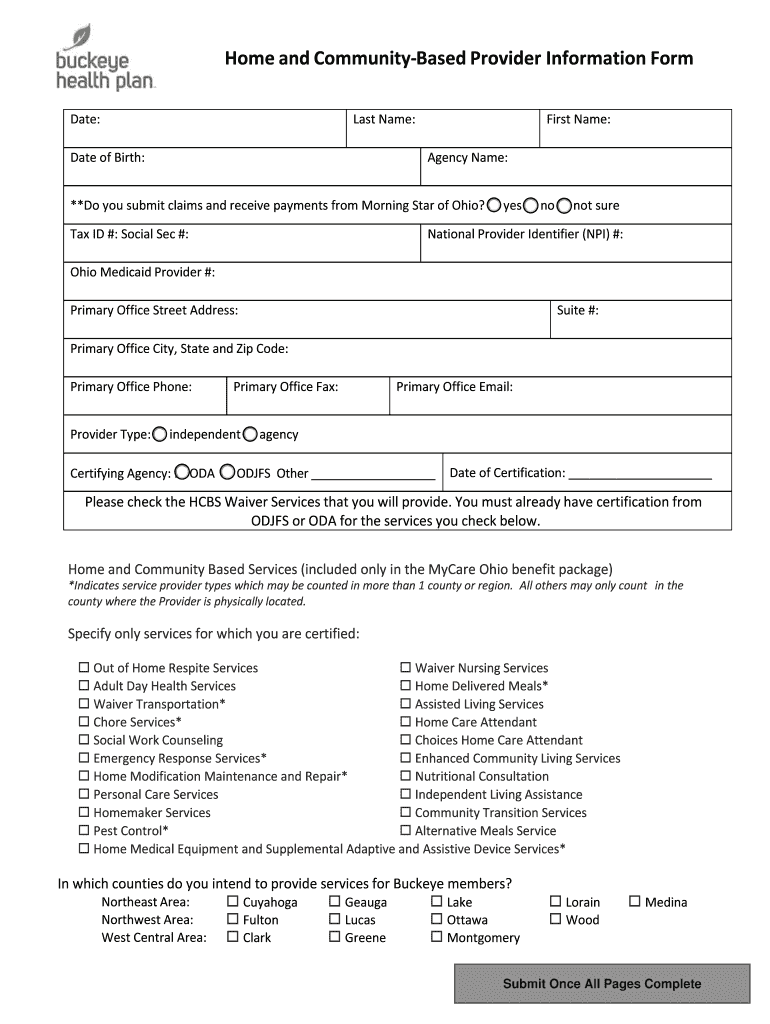
Buckeye Waiver Fill Out and Sign Printable PDF Template signNow
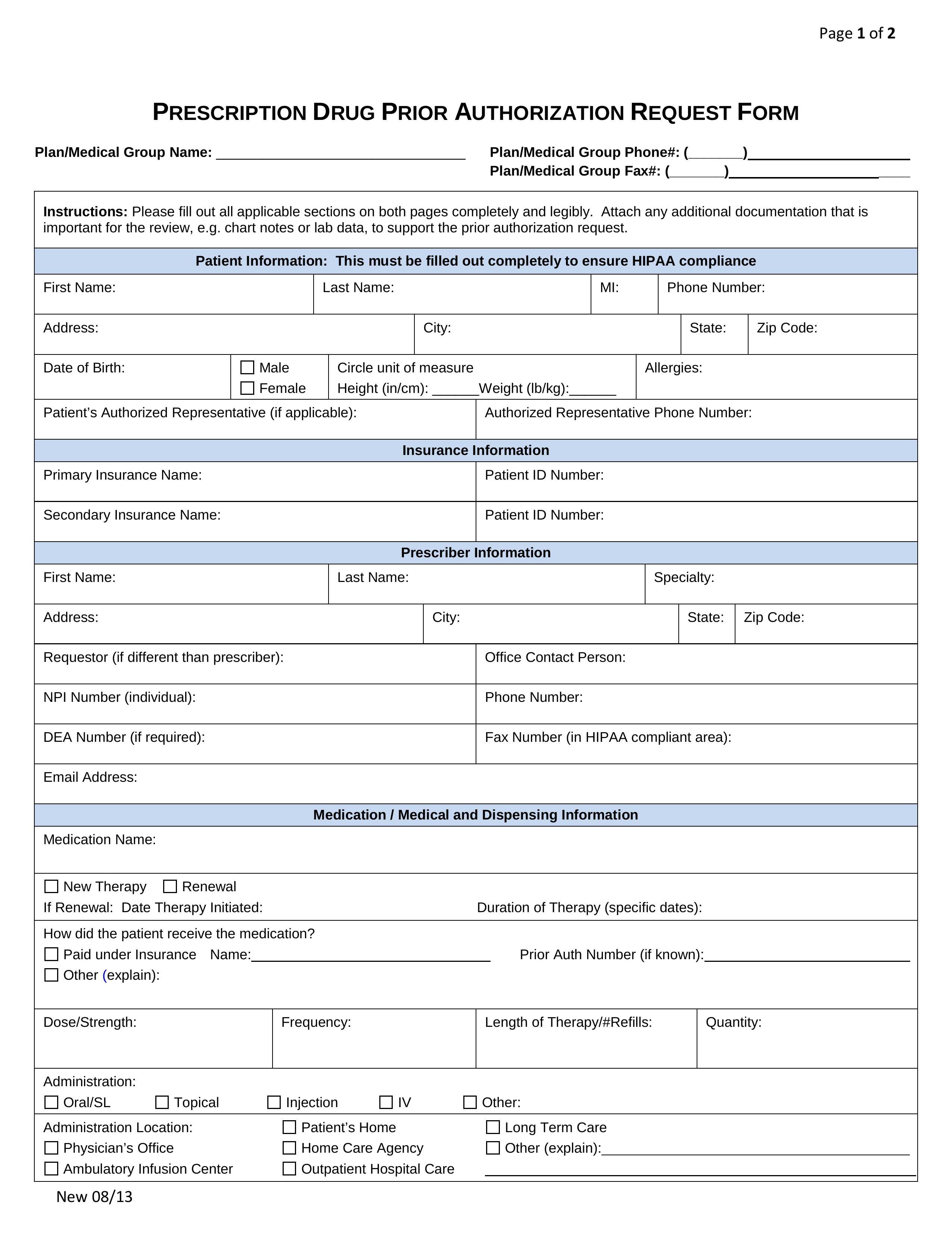
Indicates required field member information member id * date of birth last name, first(mmddyyyy). Edit your buckeye mycare prior authorization form online type text, add images, blackout confidential details, add comments, highlights and more. We call this prior authorization(pa). Web complete buckeye mycare prior authorization form online with us legal forms. Web ambetter prior authorization request form.

PDF Format Prior Authorization Form Sample Templates
Web ambetter prior authorization request form. Web requesting physician to receive priority. Save time and complete online. Web complete buckeye mycare prior authorization form online with us legal forms. Prior authorization does not guarantee.
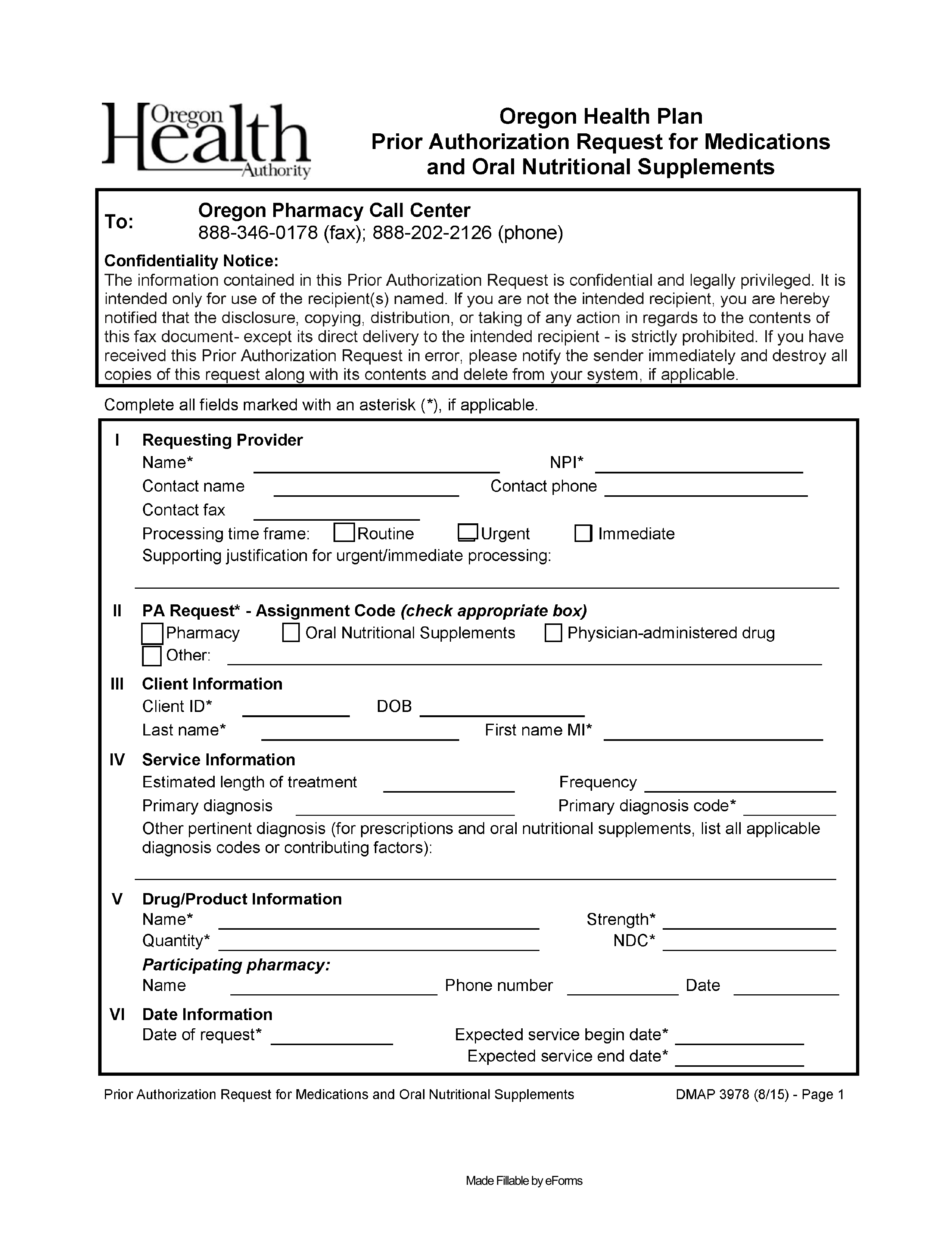
Free Oregon Medicaid Prior Authorization Form PDF eForms
Determination within 10 calendar days of receiving all necessary information. We call this prior authorization. Sign it in a few. Prior authorization does not guarantee. Web outpatient complete and fax to:
If You Don’t Get Approval, You.
Indicates required field member information member id * date of birth last name, first(mmddyyyy). Sign it in a few. We call this prior authorization(pa). If your drug needs prior authorization, call buckeye health plan.
We Require You To Get Approval From Us Before We Agree To Cover Certain Drugs.
Web ambetter prior authorization request form. Save time and complete online. The process of getting prior approval from buckeye as to the appropriateness of a service or medication. Web you must get our okay for certain drugs before using them.
Edit Your Buckeye Mycare Prior Authorization Form Online Type Text, Add Images, Blackout Confidential Details, Add Comments, Highlights And More.
Web requesting physician to receive priority. Easily fill out pdf blank, edit, and sign them. Determination within 10 calendar days of receiving all necessary information. Web medication prior authorization request form buckeye community health plan, ohio (do not use this form for biopharmaceutical products) fax this completed.
We Call This Prior Authorization.
Please click view all or search by generic or brand name to find the correct prior authorization fax form for. Web outpatient complete and fax to: Use our preferred drug list to find more information on. Save or instantly send your ready documents.