Ssa Form 1763
Ssa Form 1763 - If you send me your zip code, i will find the phone number and address of social security office nearer to you. Web the completion of this form is needed to document your voluntary request for termination of medicare coverage as permitted under the code of federal regulations. Web to apply in person or by phone, find and contact your local social security office. Not all forms are listed. Name of worker on whose account benefits are being paid. Page 1 of 3 omb no. Request for termination of premium part a, part b, or part b immunosuppressive drug coverage. Having filled it out completely, the applicant should submit it to the applicant's local ssa office. Many types of health care providers accept medicare. All forms are printable and downloadable.
Web all forms are free. Section 1838(b) and 1818a(c)(2)(b) of the social security act require filing of notice advising the administration when termination of medicare coverage is requested. You’ll need to complete the form during an interview with a representative of the social security administration (ssa) by phone or in person. Page 1 of 3 omb no. If you download, print and complete a paper form, please mail or take it to your local social security. Having filled it out completely, the applicant should submit it to the applicant's local ssa office. People with medicare premium part a or b who would like to terminate their hospital or medical. Web the cms 1763 form must be completed during or after an interview with a representative from the social security administration. Use fill to complete blank online medicare & medicaid pdf forms for free. Who can use this form?
Many types of health care providers accept medicare. Web all forms are free. Name of worker on whose account benefits are being paid. Web the completion of this form is needed to document your voluntary request for termination of medicare coverage as permitted under the code of federal regulations. If you send me your zip code, i will find the phone number and address of social security office nearer to you. Find a doctor, care provider, or hospital that accepts medicare. Request for termination of premium part a, part b, or part b immunosuppressive drug coverage. Not all forms are listed. All forms are printable and downloadable. People with medicare premium part a or b who would like to terminate their hospital or medical.

Ssa 1724 Printable Form Printable Word Searches
Who can use this form? Page 1 of 3 omb no. Request for termination of premium part a, part b, or part b immunosuppressive drug coverage. Once completed you can sign your fillable form or send for signing. Name of worker on whose account benefits are being paid.
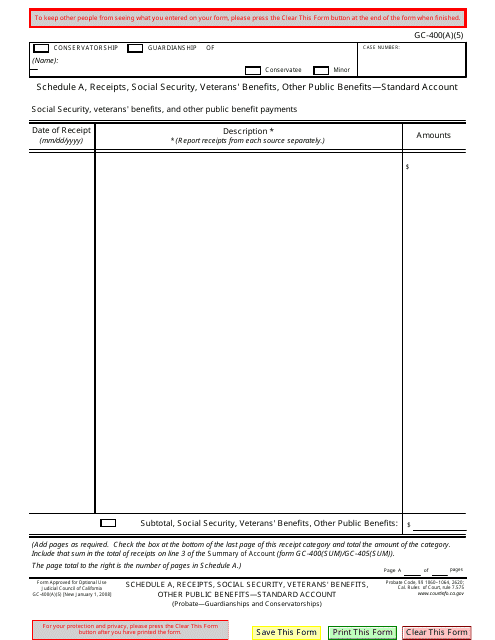
Form GC400(A)(5) Schedule A Download Fillable PDF or Fill Online
Who can use this form? Find a doctor, care provider, or hospital that accepts medicare. You’ll need to complete the form during an interview with a representative of the social security administration (ssa) by phone or in person. Web the completion of this form is needed to document your voluntary request for termination of medicare coverage as permitted under the.

Download Form SSA 1696 for Free Page 6 FormTemplate
All forms are printable and downloadable. Many types of health care providers accept medicare. You’ll need to complete the form during an interview with a representative of the social security administration (ssa) by phone or in person. People with medicare premium part a or b who would like to terminate their hospital or medical. Web to apply in person or.
Where Do I Mail Medicare Form Cms 1763 Form Resume Examples AjYdXvKoYl
Name of worker on whose account benefits are being paid. If you send me your zip code, i will find the phone number and address of social security office nearer to you. Once completed you can sign your fillable form or send for signing. Not all forms are listed. For additional information, go to.
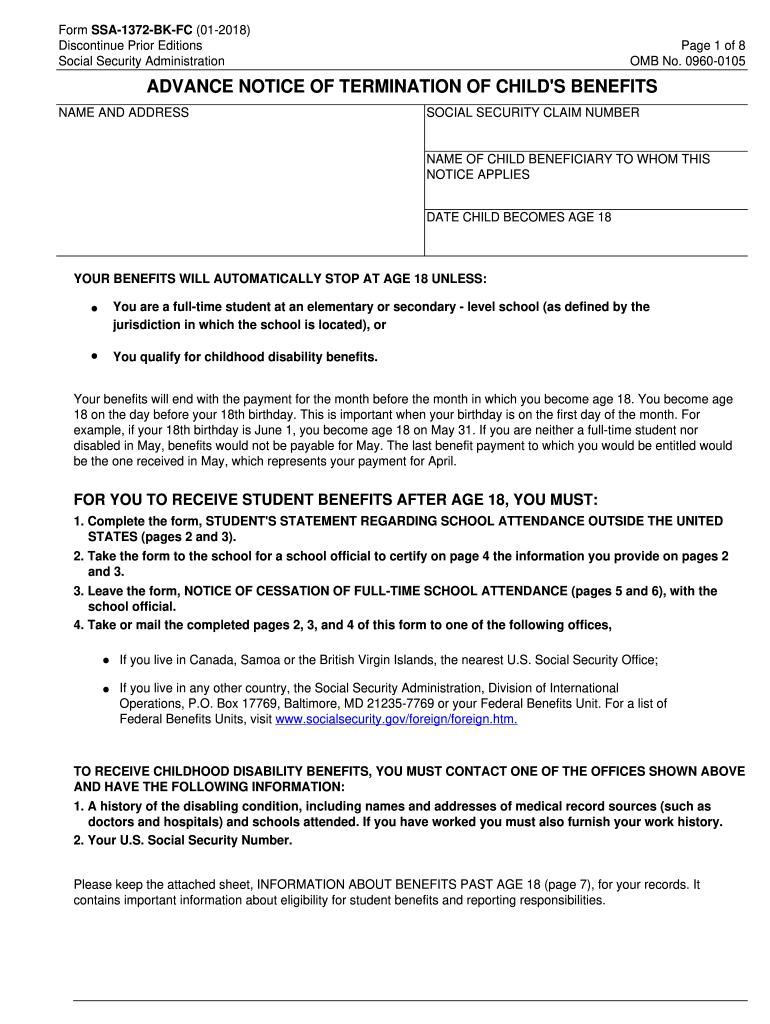
SSA1372BKFC 20182022 Fill and Sign Printable Template Online US
Not all forms are listed. People with medicare premium part a or b who would like to terminate their hospital or medical. Name of worker on whose account benefits are being paid. Having filled it out completely, the applicant should submit it to the applicant's local ssa office. Use fill to complete blank online medicare & medicaid pdf forms for.
Where Do I Mail Medicare Enrollment Application
If you send me your zip code, i will find the phone number and address of social security office nearer to you. Page 1 of 3 omb no. Web the completion of this form is needed to document your voluntary request for termination of medicare coverage as permitted under the code of federal regulations. Web the cms 1763 form must.
Form SSA1696 Supplement 1 Download Fillable PDF or Fill Online
Find a doctor, care provider, or hospital that accepts medicare. Web the completion of this form is needed to document your voluntary request for termination of medicare coverage as permitted under the code of federal regulations. All forms are printable and downloadable. Name of worker on whose account benefits are being paid. For additional information, go to.

CMS 1763 How to opt out of your medicare insurance
Web to apply in person or by phone, find and contact your local social security office. Not all forms are listed. Once completed you can sign your fillable form or send for signing. Web the completion of this form is needed to document your voluntary request for termination of medicare coverage as permitted under the code of federal regulations. Web.
Medicare Part B Form Cms 1763 Form Resume Examples X42M4aXaVk
You’ll need to complete the form during an interview with a representative of the social security administration (ssa) by phone or in person. Who can use this form? Section 1838(b) and 1818a(c)(2)(b) of the social security act require filing of notice advising the administration when termination of medicare coverage is requested. Once completed you can sign your fillable form or.
Form SSA1696 Fill Out, Sign Online and Download Fillable PDF
Many types of health care providers accept medicare. All forms are printable and downloadable. Not all forms are listed. Once completed you can sign your fillable form or send for signing. Name of worker on whose account benefits are being paid.
All Forms Are Printable And Downloadable.
Once completed you can sign your fillable form or send for signing. For additional information, go to. People with medicare premium part a or b who would like to terminate their hospital or medical. Request for termination of premium part a, part b, or part b immunosuppressive drug coverage.
Having Filled It Out Completely, The Applicant Should Submit It To The Applicant's Local Ssa Office.
If you download, print and complete a paper form, please mail or take it to your local social security. Web all forms are free. Who can use this form? Page 1 of 3 omb no.
Use Fill To Complete Blank Online Medicare & Medicaid Pdf Forms For Free.
Web to apply in person or by phone, find and contact your local social security office. Name of worker on whose account benefits are being paid. If you send me your zip code, i will find the phone number and address of social security office nearer to you. Web the cms 1763 form must be completed during or after an interview with a representative from the social security administration.
You’ll Need To Complete The Form During An Interview With A Representative Of The Social Security Administration (Ssa) By Phone Or In Person.
Many types of health care providers accept medicare. Find a doctor, care provider, or hospital that accepts medicare. Not all forms are listed. Section 1838(b) and 1818a(c)(2)(b) of the social security act require filing of notice advising the administration when termination of medicare coverage is requested.